
I Was a Perfect Nurse For 25 Years Until My New Boss Framed Me For Theft—Then I Discovered His Shocking Secret
I Was a Perfect Nurse For 25 Years Until My New Boss Framed Me For Theft—Then I Discovered His Shocking Secret
Twenty-Five Years Without a Single Day
I finished charting at 6:47 in the morning, the same way I'd finished thousands of shifts before — pen down, clipboard squared, one last walk through the ward to make sure everything was exactly as it should be. Twenty-five years. Not a single absence. Not one missed shift, not one late call-in, not even during the winter my mother passed and I drove four hours to the funeral and four hours back and showed up the next evening in clean scrubs with my hair pinned up like nothing had happened. St. Jude's Memorial wasn't just where I worked. It was where I'd learned to be the kind of nurse I'd always wanted to be — the kind who remembered which patients were afraid of needles, who kept a spare pair of reading glasses in her pocket for the elderly folks who couldn't read their discharge instructions. I'd trained half the floor staff currently on rotation. I'd held hands through diagnoses that changed lives in an instant. The hallway was quiet at that hour, the overnight hum of monitors and soft-soled shoes settling into the particular stillness that only exists just before a hospital wakes up. I stood there for a moment longer than I needed to, breathing it in. Twenty-five years of that smell — antiseptic and floor wax and something underneath it all that I could only call purpose — and it still felt like mine.
 Image by RM AI
Image by RM AI
The New Director Arrives
The board sent the announcement on a Tuesday, and by Wednesday morning the break room was already buzzing. Marcus Brennan. Thirty-four years old. A resume that read more like a corporate consulting portfolio than a healthcare leadership track — cost optimization, operational restructuring, revenue cycle management. The kind of language that sounds impressive until you've spent two decades watching what happens when a hospital starts treating patients like line items. I attended the introductory meeting with the other department heads, sitting near the back with my coffee going cold in my hand. Marcus walked in wearing a suit that probably cost more than my monthly take-home, dark hair perfectly in place, and he smiled at the room the way people smile when they've already decided what they think of you. His presentation was polished. I'll give him that. Slides full of benchmarks and performance gaps and something he kept calling 'strategic realignment.' Around me, I could see the other senior staff shifting in their seats — small movements, the kind people make when they're trying not to look at each other. I kept my expression neutral and my pen moving across my notepad. He was new. New directors always came in with big language and bold charts. Most of them settled down once they understood how a floor actually ran. But by the time he wrapped up, he had used the phrase 'operational efficiency' three times, and something about the way he said it made the back of my neck prickle.
 Image by RM AI
Image by RM AI
Efficiency Initiatives
The first round of changes arrived in our inboxes two weeks after Marcus's introductory meeting — new supply ordering protocols, centralized purchasing approvals, and a request from administration for detailed staffing cost analyses broken down by department, seniority tier, and overtime hours. I filled out every form. I submitted every report on time, formatted exactly the way the new templates required. That was just how I operated. If there were new rules, I followed them. I'd outlasted four directors before Marcus, and I'd learned that the fastest way to get through a transition period was to be the person nobody had a reason to look at twice. But the changes kept coming. Weekly budget check-ins. Supply usage audits. A new approval chain for anything over fifty dollars. The younger nurses seemed to take it in stride — most of them had never known anything different, had come up through systems that already ran this way. For those of us who'd been here long enough to remember when a charge nurse could order what her patients needed without filling out a three-page justification form, it felt like something was being slowly rearranged around us. Marcus ran the department head meetings with the same polished efficiency he'd brought to that first presentation. He was never rude. He was never unreasonable. He just kept asking questions that had numbers as their only acceptable answers. After each meeting, the hallway outside the conference room held a particular kind of quiet — not peaceful, just careful.
 Image by RM AI
Image by RM AI
The First Departures
Sandra from the cardiac unit was the first to go. She'd been at St. Jude's for twenty-two years, and she announced her early retirement at the end of a Thursday staff meeting with a smile that didn't quite reach her eyes. Two weeks later, Paul from orthopedics followed, and then Miriam from the ICU, and suddenly we were throwing three farewell parties in the same month. I went to all of them. I brought the same sheet cake from the bakery on Clement Street that I always brought to these things, and I stood in the break room making conversation while the honorees said things like 'it just felt like the right time' and 'I'm looking forward to the next chapter.' I hugged them and meant it. But I also noticed that none of them said much about why, specifically, now. The replacements came quickly — younger nurses, capable enough, but hired at salary grades that were noticeably lower than the positions they were filling. I told myself that was just how healthcare worked these days. Budgets were tight everywhere. Early retirement packages were a reasonable tool. I had no proof of anything except that three people I'd worked alongside for decades were suddenly gone, and the break room felt different without them. The monthly all-staff meeting that followed had three empty chairs where Sandra, Paul, and Miriam used to sit, and I found myself looking at those chairs longer than I meant to.
 Image by RM AI
Image by RM AI
Under the Microscope
It started with one unannounced visit, then two, then enough that the night shift staff stopped being surprised when Marcus appeared at the end of the corridor with his tablet in hand. He'd show up around two in the morning, sometimes later, moving through the floor with that same measured calm he brought to every meeting. He asked about staffing ratios. He asked about supply usage per patient hour. He asked how we handled overtime authorization when census spiked unexpectedly. I answered every question the same way I answered everything — directly, with specifics, without apology. My numbers were good. My documentation was clean. If he was looking for inefficiencies in my department, he wasn't going to find them. But I'd be lying if I said his visits didn't get under my skin a little. There's a particular kind of attention that doesn't feel like interest — it feels like inventory. Like someone walking through a room and quietly calculating what things are worth. I couldn't point to anything specific he'd said or done that crossed a line. He was always professional. Always polite. I just noticed that his visits to my floor were more frequent than what I heard about from the other departments. I told myself I was probably reading into it. Then one night, near the end of a quiet shift, I turned the corner toward the supply corridor and found Marcus standing outside the blood bank at three in the morning.
 Image by RM AI
Image by RM AI
The Salary Comment
The budget review meeting was scheduled for a Friday afternoon, just the two of us in the small conference room off the administrative wing. Marcus had a printed report waiting on the table when I arrived — comparative salary data for the nursing department, broken down by years of service and hourly cost. He walked me through it the way you'd walk someone through a weather forecast. Calm. Factual. He talked about the cost differential between senior staff and newer hires, about what the numbers looked like when you projected them out over a fiscal year, about the pressure the board was putting on every department to find what he called 'creative solutions for sustainable staffing.' He never said my name. He never pointed at a specific line on the page. He didn't have to. He was talking about a senior charge nurse with twenty-five years of service, night shift, with a salary in the upper tier of the nursing pay scale. There was only one person in this hospital that description fit. I kept my hands flat on the table and my expression even. I asked clarifying questions. I took notes. I thanked him for his time when the meeting ended and walked out of that room with my back straight and my breathing steady. It wasn't until I was in the elevator that I let myself look down at the figure he'd cited — and it matched my exact salary to the dollar.
 Image by RM AI
Image by RM AI
Working Harder
After that meeting, I stopped leaving on time. I started arriving forty minutes before every shift to review the previous team's notes, and I stayed until every piece of documentation was complete and cross-checked. I volunteered for the infection control committee. I submitted a proposal for a new patient handoff protocol that administration had been talking about for two years without anyone actually writing it up. My shift reports got longer, more detailed, more airtight than they'd ever been. I told myself it was just good practice. That any charge nurse worth her badge should be operating this way. But I knew, somewhere underneath the professional logic, that I was building a record — something that would be hard to argue with if it ever came to that. I didn't know what 'that' looked like yet. I just had a bad feeling I was going to find out. I kept my head down and my work clean and tried not to let the unease show on the floor, because the last thing my team needed was to pick up on my anxiety. It was a Tuesday evening when I passed Marcus in the administrative corridor near the director's office. His door was cracked open and his voice carried just enough for me to catch a few words before I was past it — something about a timeline, something about things being handled. And then, clearly enough that I stopped walking: 'the Miller situation will resolve itself soon.'
 Image by RM AI
Image by RM AI
Thursday Morning Exhaustion
The shift that Thursday was the kind that strips something out of you. We came in short-staffed — two nurses out sick with no replacements available — and by midnight we had our first code, a sixty-three-year-old post-surgical patient whose pressure dropped without warning. We got him back. An hour later, a second code in the step-down unit, and then a trauma transfer that arrived with incomplete paperwork and a family in the waiting room who needed answers nobody had yet. I ran on adrenaline and muscle memory, the way you do after twenty-five years of nights like this. By the time the morning shift came through the doors, I had been on my feet for nearly thirteen hours straight. I finished my documentation sitting at the nurses' station while the day crew settled in around me, the parking lot outside the window going from black to gray to the pale gold of early morning. I was thinking about nothing except my car and my bed and maybe a piece of toast when I finally gathered my bag and my jacket and stood up. My pager went off before I reached the door. I looked down at the small screen, expecting a routine handoff question from the incoming charge nurse. It was a message from Human Resources, marked urgent, requesting my immediate presence in the HR suite before I left the building.
 Image by RM AI
Image by RM AI
The Closed-Door Meeting
I didn't even stop to change out of my scrubs. Thirteen hours on my feet and I walked straight from the nurses' station to the elevator, my bag still over my shoulder, my badge still clipped to my chest. The HR suite was on the third floor, and I remember the elevator doors opening and the hallway feeling quieter than it should have at that hour — that particular kind of quiet that doesn't feel like calm. The conference room door was already open. Rita was seated at the head of the table in a dark blazer, her reading glasses on their chain, a folder centered in front of her like it had been placed there with a ruler. She looked up when I came in, and something in her expression shifted — not quite guilt, not quite pity, but something uncomfortable that she was working hard to keep neutral. Then I noticed Marcus sitting to her right, and that stopped me for half a second. He was in a suit at this hour, perfectly put together, hands folded on the table. I couldn't think of a single routine HR matter that would require the director of operations to be present. I took the chair across from them and set my bag on the floor. Neither of them spoke right away. The silence in that room settled over everything like a held breath, and I sat there waiting inside it.
 Image by RM AI
Image by RM AI
The Accusation
Marcus opened the meeting without any preamble. He said that a forensic audit had uncovered evidence of systematic theft from the hospital's controlled supply inventory, and that the evidence pointed directly to me. I heard the words, but for a moment they didn't connect to anything real. I actually looked behind me, some reflex I couldn't explain, as if he might be addressing someone else. Rita slid a printed summary across the table and began reading from it in a careful, procedural voice — unauthorized extractions, misappropriation of high-value medical supplies, a pattern spanning several months. Marcus mentioned the blood bank specifically. He mentioned plasma inventory. He used the phrase 'systematic misappropriation' twice, and each time it landed like something physical. I kept waiting for the part where this would make sense, where someone would explain there had been a mistake or a mix-up in the records. That part didn't come. Rita turned a page and read language about the formal investigation process, about the hospital's obligation to report findings to the state licensing board, about the possibility of referral for criminal prosecution. That last phrase — criminal prosecution — left the room and just hung there in the air between us, and I sat very still, unable to move, unable to speak, unable to make the words mean anything other than exactly what they meant.
 Image by RM AI
Image by RM AI
The Fabricated Evidence
Marcus opened the folder and turned it to face me. The first page was a forensic audit report, dense with timestamps and transaction codes. He flipped through it slowly, and I watched page after page go by — inventory extraction logs, digital access records, lab chain-of-custody forms. Each document was formatted with the hospital's official header. Each one looked exactly like the kind of paperwork I had generated and reviewed thousands of times over twenty-five years. The extractions were all timestamped during night shift hours, the hours I worked. The access logs showed a single employee credential authorizing every transaction. Marcus pointed to the top of one page and said the credential number was mine. I looked at it. It was my number. I knew my employee ID the way I knew my own handwriting — I had typed it into systems so many times it was automatic — and the number on that page was correct. It appeared on every single log in that folder. Dozens of entries. Six months of records. The total value of missing plasma ran into figures that made my stomach drop. Rita kept her eyes on her notepad. Marcus watched me read. I turned the pages carefully, the way I would turn a patient chart when something wasn't adding up, looking for the error, looking for the place where this stopped being real. My employee ID number stared back at me from every page, and I couldn't find the place where it stopped.
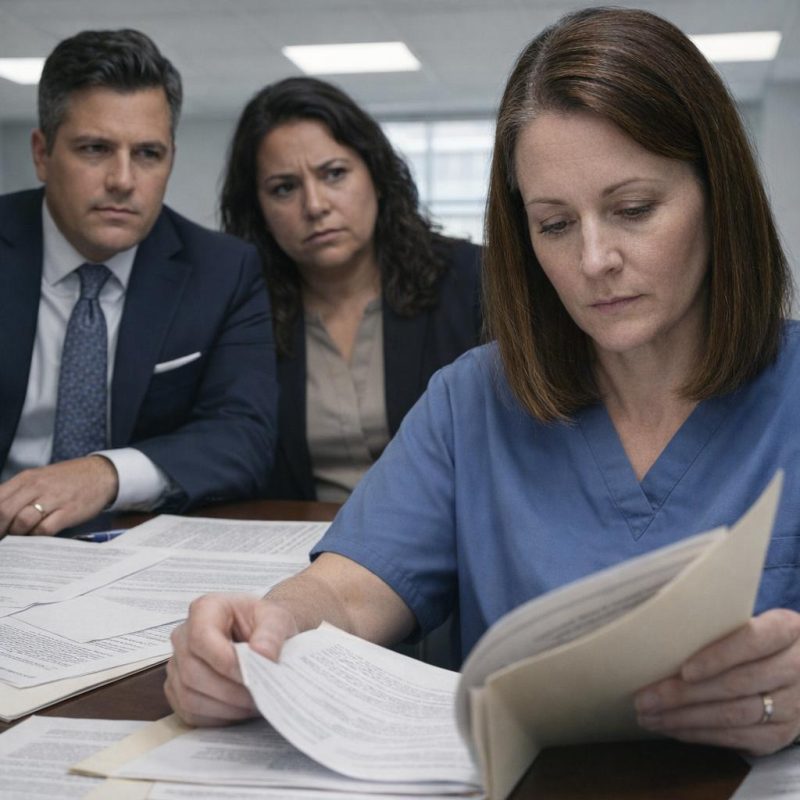 Image by RM AI
Image by RM AI
The Forced Resignation
Marcus reached into a second folder and slid a single sheet of paper across the table toward me. It was a resignation letter, already drafted, with my name typed at the top and a signature line at the bottom. He said signing it was the most straightforward path forward. He said it would allow the hospital to handle the matter internally, that it would reduce the likelihood of a formal referral to the licensing board, that it would preserve what he called 'some professional dignity.' Rita explained the alternative in the same careful procedural voice she'd used all morning — a formal disciplinary hearing, mandatory reporting to the state, the full investigative process. Marcus said the evidence was conclusive and that prolonging things would only make them worse. I stared at that piece of paper. Part of me wanted to pick it up just to have something to hold onto, some way to make the pressure in that room stop. Twenty-five years. Two codes last night alone. I had given this hospital everything I had, and now there was a pre-written letter sitting in front of me asking me to say I had stolen from it. I reached out and my fingers touched the edge of the paper. Then I pulled my hand back and set it flat on the table.
 Image by RM AI
Image by RM AI
Demanding Time
I took a breath and made myself speak slowly. I said I would not be signing anything that morning. Marcus started to respond and I kept going — I said I was invoking my right to union representation, that I was requesting forty-eight hours to review the evidence in full before any further action was taken, and that I wanted copies of every document in that folder. The room went very quiet. Rita looked at Marcus, then back at me, and said that union procedures did allow for that request. Marcus's expression didn't change much, but something tightened around his jaw. He said the delay wouldn't alter the outcome. I said I understood his position. Rita confirmed the forty-eight-hour window in writing, initialing the bottom of her notepad page, and said copies of the documentation would be prepared for me before I left the building. Marcus gathered the folder without another word. I signed the acknowledgment form confirming I had been informed of the allegations — not the resignation letter, just the acknowledgment — and pushed it back across the table. Nobody spoke after that. Rita stood and said she would have the copies ready within the hour. I nodded and sat with my hands folded in my lap, and the room held its quiet around me like something that had been waiting a long time to settle.
 Image by RM AI
Image by RM AI
Glen Arrives
I texted Glen from the elevator before I even reached the lobby. He called me back before I made it to the cafeteria. I found a corner table near the back, away from the morning rush of staff coming off night shift, and I sat down with the copied folder in front of me and waited. Glen arrived twelve minutes later, still pulling on his jacket, his worn briefcase under one arm. He sat across from me and didn't say anything at first — just looked at my face and then at the folder, and then he said, 'Walk me through all of it.' So I did. I told him everything from the pager message to the resignation letter to the forty-eight-hour window. He listened without interrupting, turning pages as I talked, his reading glasses low on his nose. When I finished he was quiet for a moment. Then he said the charges were serious and that we needed to treat them that way, not because he thought I had done anything wrong, but because the documentation looked thorough and whoever had put it together had been careful. He outlined my rights under the union contract, explained what the hospital could and couldn't do during the review period, and told me to go home and go through every page of those copies myself — cross-reference the timestamps, check the access logs, look for anything that didn't match what I actually knew about how those systems worked. I walked out of that cafeteria still frightened, but I wasn't carrying it alone anymore, and that was the first thing in hours that felt like solid ground.
 Image by RM AI
Image by RM AI
Studying the Documents
I got home just after nine in the morning, still in my scrubs, and I didn't sleep. I made coffee, cleared the kitchen table, and spread every copied page out in the order Marcus had presented them. Then I started at the beginning. I read the way I read patient charts when something felt wrong — slowly, methodically, not looking for what I expected to find but looking for what was actually there. I cross-referenced the extraction timestamps against my own shift schedule, which I had printed from the employee portal before leaving the hospital. Every single logged transaction fell within my documented work hours. The digital access signatures looked exactly like the system-generated records I had seen thousands of times. The chain-of-custody forms were formatted correctly. Whoever had assembled this had known what they were doing. I was two hours in and my coffee had gone cold when I reached the section on plasma product specifications. The lot numbers were listed in a column on the right side of each extraction log, long alphanumeric strings that identified the specific plasma sub-type involved. I had ordered blood bank products for twenty-five years. I knew the standard lot number formats for every product we stocked in our emergency department. I ran my finger down the column slowly, and something snagged — the prefix codes on these lot numbers didn't match any plasma product format I had ever ordered or signed for.
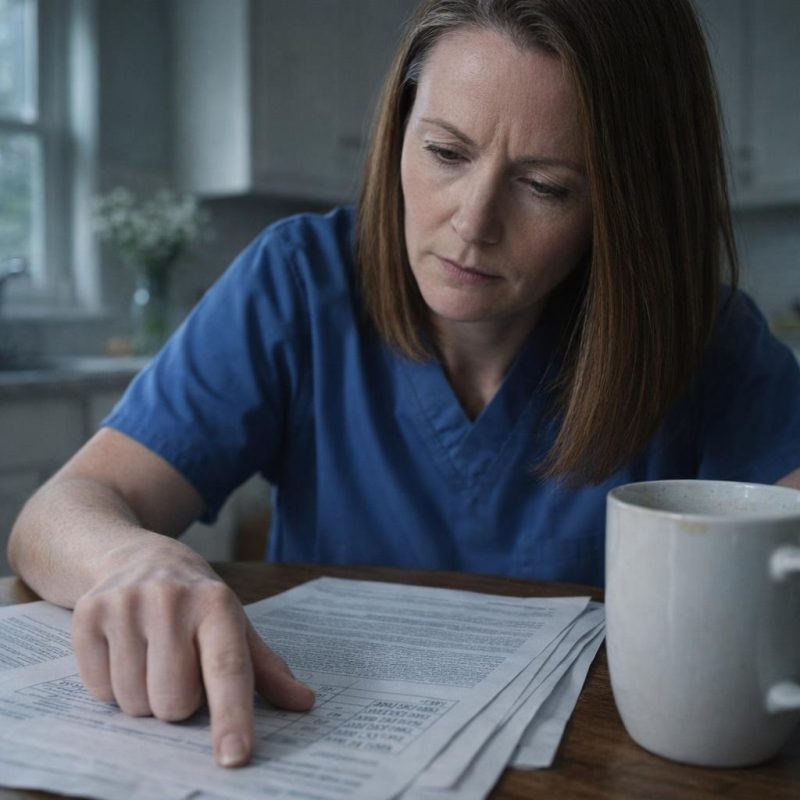 Image by RM AI
Image by RM AI
The Rare Plasma
I pulled up the hospital's internal blood bank inventory catalog on my laptop — the same system I had used on night shift for years — and I searched the plasma sub-type listed in the extraction logs. Nothing came back. I searched the product prefix code. Nothing. I went to the regional blood bank supplier database that the hospital used for special orders and ran the same search. The sub-type existed, but the catalog entry was flagged: highly specialized, limited clinical application, not stocked at standard emergency facilities, requires institutional authorization and a documented clinical protocol to order. I sat back and read that entry twice. Then I pulled up St. Jude's standing inventory list — the official document that specified every blood product the hospital was authorized to carry — and I went through it line by line. The plasma sub-type from the extraction logs did not appear anywhere on it. Not in emergency stock. Not in surgical reserves. Not in any specialty unit. The hospital did not carry this product. According to every database I could access, St. Jude's had never carried it. The extraction logs described the theft of a plasma product that this hospital's inventory system showed we didn't stock.
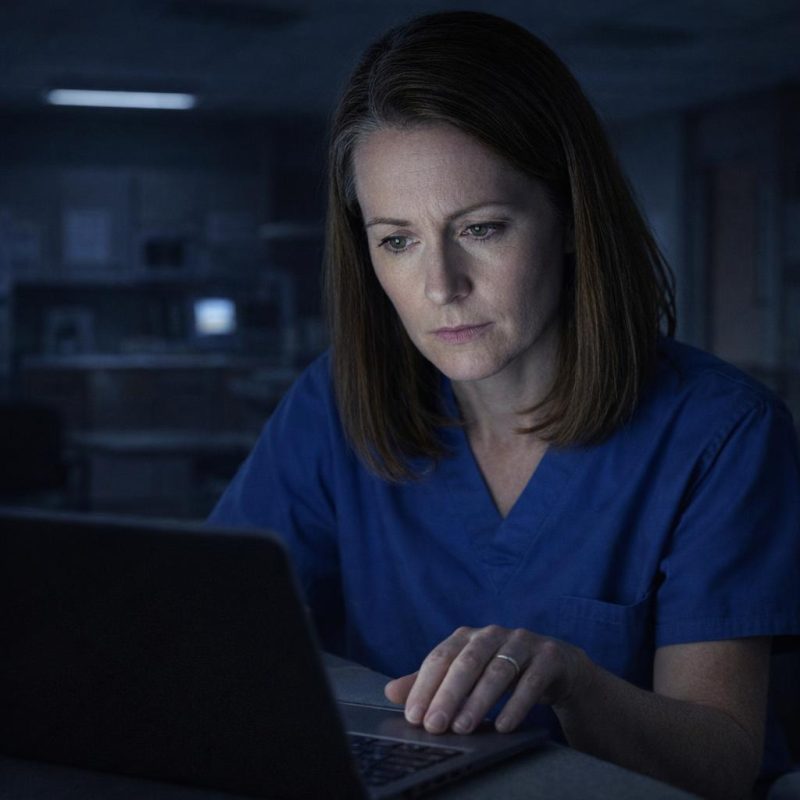 Image by RM AI
Image by RM AI
Trusting My Experience
It was past midnight when I finally picked up the phone and called Glen. I knew it was late, but I also knew he'd told me to call whenever I found something — and what I'd found couldn't wait until morning. He picked up on the third ring, voice rough but alert, and I walked him through everything: the plasma sub-type, the lot numbers, the supplier database flags, the fact that St. Jude's standing inventory list had never included this product. I could hear him go quiet on the other end, the kind of quiet that meant he was thinking hard. I told him the extraction logs described a theft of something we didn't stock, something that would have required institutional authorization just to order in the first place. He asked me to slow down and repeat the part about the catalog flags. I did. He asked about the standing inventory document — whether it was the official version, whether it was dated. I told him yes on both counts. Another long pause. Then he said that whoever put those logs together didn't know how a blood bank actually works. I told him that was exactly what I thought. His voice came back flat and certain: "Diane, this means someone is framing you."
 Image by RM AI
Image by RM AI
Refusing to Sign
Glen and I walked into that HR office the next morning side by side, and I made sure I was the one who spoke first. Rita was already seated, reading glasses on, a folder open in front of her. Marcus stood near the window in that expensive suit of his, arms crossed, expression perfectly composed. Rita slid the resignation papers across the table toward me. I didn't touch them. I told her I wasn't signing anything. I set down the printed pages I'd brought — the supplier database entry, the standing inventory list, the catalog flags — and I explained, calmly and in plain language, that the plasma sub-type listed in the extraction logs was a product St. Jude's had never been authorized to carry. Glen backed me up immediately, citing the union's right to challenge evidentiary basis before any disciplinary action could proceed. Marcus barely glanced at my documents. He said it was probably a clerical error in the system, that these things happened, that it didn't change the core findings. Rita shifted in her chair and didn't say anything. I told Marcus I wanted full access to the pharmaceutical system logs to verify the discrepancy myself. He paused just long enough to be noticeable, then said I could have limited supervised access. I thanked him in a voice that didn't sound like gratitude at all, and I meant every word of it exactly that way.
 Image by RM AI
Image by RM AI
Planning the Audit
Glen came back to my apartment that afternoon with his worn briefcase and a legal pad, and we spread everything across the kitchen table. He'd done this kind of documentation work before — grievance cases, wrongful terminations — and he knew which records would hold up and which ones would get thrown out on a technicality. We started by mapping the database layers: the extraction logs I'd already pulled, the pharmaceutical transfer records I hadn't accessed yet, and the authorization logs that would show who signed off on what and when. Glen explained that my master administrative credentials, the ones I'd held for eleven years, gave me legitimate read access to most of those layers without triggering a security flag. That mattered. We weren't doing anything improper, and we needed the paper trail to show that clearly. I wrote out a timeline — which records to pull first, which cross-references to run, how to document each finding with a timestamp and a source notation. Glen reviewed it and added two steps I hadn't thought of: a chain-of-custody note for every screenshot, and a running log of my own shift hours to establish where I physically was during any suspicious entries. By the time he left, the legal pad was full and the kitchen table looked like a command center. I sat with the plan in front of me for a long time after he was gone, and something in my chest had gone still and steady.
 Image by RM AI
Image by RM AI
The Night Audit Begins
I went in for my regular night shift and kept everything exactly as normal as I could manage. I took report, checked my patients, did my rounds. The floor settled into its usual rhythm around two in the morning — call lights quiet, the charge nurse doing paperwork at the far end of the station, the hallways dim and unhurried. I sat down at the workstation in the medication room, the one with the least foot traffic, and I logged into the pharmaceutical database using my administrative credentials. My hands were steadier than I expected. I pulled up the lot numbers from the extraction logs — the ones that described the plasma sub-type St. Jude's had never stocked — and I ran them through the transfer records layer. The first search came back empty. I adjusted the date range and ran it again. This time entries appeared, several of them, each one tagged with a transfer status rather than a waste or destruction code. I opened the first record and read through it carefully. The plasma hadn't been discarded. It hadn't been returned to a supplier. According to the database, it had been moved — logged as an outbound transfer, timestamped, assigned a destination code I didn't recognize, and marked as completed.
 Image by RM AI
Image by RM AI
Following the Digital Trail
I worked through the rest of that night the same way I'd worked every difficult shift in twenty-five years — methodically, one step at a time, not letting myself get ahead of the data. I pulled each lot number individually and traced it through the transfer records layer, then cross-referenced the timestamps against the extraction log entries. Every single unit matched. Every extraction had a corresponding outbound transfer record, logged within hours, all of them assigned the same unfamiliar destination code. I documented each finding the way Glen had shown me: screenshot, source notation, timestamp, my own shift log entry for that hour. The destination code appeared consistently across six months of records — not scattered, not random, but regular. Weekly, sometimes twice weekly, always the same code. I didn't know what the code pointed to yet. I wrote it down each time it appeared anyway, because patterns matter before you understand them. Around four in the morning a call light went on in room seven and I went and took care of it, checked vitals, reassured my patient, came back and kept going. By the time the day shift started arriving, I had fourteen pages of notes and a folder of screenshots organized by date. I closed the database, logged out cleanly, and sat for a moment with the folder in my lap, feeling the weight of what I'd built through the night.
 Image by RM AI
Image by RM AI
Master Key Access
The second night I went deeper. I used my master administrative keys to access the restricted authorization logs — the layer that recorded who had approved each transfer, not just that a transfer had occurred. I typed in my employee ID as a search parameter, expecting to find nothing, expecting my credentials to come up clean. The results loaded and I sat very still. My employee ID was attached to every single suspicious transfer. Every one. The authorization signatures on those outbound records bore my name, my ID number, my digital credentials. I opened the timestamp details on the first entry and checked it against my own shift log. I had been in a patient room at that hour — I had a vitals entry to prove it, logged from the bedside terminal. I checked the second entry. I had been on a break, off the floor, my badge scan showing me in the break room. I went through a dozen more. The authorizations had been made from a workstation I hadn't been near, during windows when my physical location was documented somewhere else entirely. Someone had used my credentials to sign off on transfers I had never seen, never approved, never knew existed. I sat there with my name on the screen in front of me, attached to dozens of transactions I had never performed, and the feeling that settled over me was something colder and quieter than anger.
 Image by RM AI
Image by RM AI
Cross-Referencing the Registry
On the third night I pulled up the hospital's off-site clinical registry — a separate database layer that tracked authorized shipments to external facilities. I entered the plasma lot numbers one by one. Every single one came back with a hit. Not flagged as missing. Not logged as stolen. Each unit appeared in the registry as a completed authorized transfer, documented with a facility code, a shipment date, and a receiving signature. The entries were clean and official-looking, formatted exactly the way a legitimate inter-facility transfer would be. I cross-referenced the facility code against the hospital's list of known affiliate locations — partner hospitals, satellite clinics, approved research sites. The code didn't appear on any of them. I ran it through the broader regional registry. Still nothing. I went back to the individual transfer entries and looked for any additional identifying information attached to the destination field. Most entries had only the code. But near the bottom of one record, in a data field that wasn't always populated, there was a physical address — a street address, a suite number, a city.
 Image by RM AI
Image by RM AI
The Second Night
I came back the following night with a cleaner focus. The address could wait — first I needed to understand the full scope of what I was looking at. I pulled the transfer records for the entire six-month window and started calculating totals. The numbers were bigger than I'd expected. Not a few units here and there. Dozens of units per week, week after week, consistent and scheduled, the way a supply contract runs rather than the way an opportunistic theft looks. I added up the cumulative volume across the full period and sat back from the screen. The quantity was substantial enough that moving it would have required cold storage logistics, coordinated pickup, documentation at both ends. I thought about the physical reality of that — the coolers, the transport protocols, the chain-of-custody requirements for blood products. One person working alone couldn't manage this. The transfer volumes logged across six months totaled far more than any single individual could have moved, stored, or coordinated without help.
 Image by RM AI
Image by RM AI
Tracking Digital Signatures
I shifted my focus from the transfer volumes to the authorization timestamps themselves. Each transfer had a digital signature attached — a credential stamp that logged who approved the movement of product and when. My login. My employee ID. My name, over and over, on forms I had never touched. I pulled up my personal calendar and cross-referenced it against the hospital's official time-off records. The first mismatch jumped out within minutes. The authorizations were spread across months, not clustered together, which made them harder to spot at a glance. Someone had been patient about this. Careful. I kept going, checking each date against my records — vacation days, conference registrations, hotel receipts still saved on my phone. The conflicts kept appearing. I printed the time-off records alongside the authorization logs and laid them side by side on the desk. The dates didn't just conflict — they were impossible. And then I found the one that stopped me cold: a transfer form bearing my digital signature, timestamped at 2:47 AM on a night I was documented as checked into a hotel four hundred miles away.
 Image by RM AI
Image by RM AI
The Transfer Pattern
I spent the next hour building a proper timeline. I took every transfer entry and plotted it out on a legal pad — date, time, volume, authorization stamp. When I stepped back and looked at the full picture, the pattern was immediate and unmistakable. Tuesday nights. Friday nights. Every single week, without exception, for six months. The transfers always fell between 2 AM and 4 AM, that narrow window when the overnight skeleton crew was at its thinnest and administrative oversight was essentially nonexistent. No random clustering, no gaps that might suggest improvisation. Just a steady, reliable rhythm, the kind you'd see in a legitimate scheduled shipment contract. I thought about what that kind of consistency required. You'd need to know the staffing rotations. You'd need to know which security checkpoints were active at 2 AM versus 4 AM. You'd need to know the cold-chain handling windows well enough to time the pickups without product degradation. This wasn't someone who had stumbled onto an opportunity. Whoever was behind this understood hospital operations from the inside — the rhythms, the gaps, the paperwork flows. I sat there with my legal pad and the neat columns of dates and times, and the sheer professional precision of what I was looking at settled over me like a weight I couldn't shake off.
 Image by RM AI
Image by RM AI
Volume Analysis
I turned to the volume numbers next, because the pattern alone wasn't the whole story. I pulled the unit counts for each transfer and started working through the storage math. Fresh frozen plasma has a strict handling window — it has to be maintained at negative eighteen degrees Celsius or colder, and once thawed it degrades fast. The quantities being moved in each shipment weren't trivial. We were talking about enough product per week that you'd need a dedicated medical-grade freezer unit, not a household chest freezer from a big-box store. You'd need backup temperature monitoring, alarm systems for power failures, trained personnel who understood the handling protocols. The cumulative six-month volume I'd calculated the night before would have required consistent, professional cold-chain management from the moment it left our blood bank to wherever it ended up. I thought about what that actually looked like in practice — the equipment costs alone would run into tens of thousands of dollars. This wasn't product being resold out of the back of a van. The destination, wherever it was, had to be a functioning medical facility with proper infrastructure. The Riverside Drive address kept coming back to me. Whatever was at that location, it wasn't a storage unit or a loading dock. It had to be something equipped to handle this properly.
 Image by RM AI
Image by RM AI
Printing the Evidence
I'd been careful up to this point, but I needed hard copies. Digital records could be altered, access logs could be wiped, and I wasn't naive enough to think my hospital login would stay active indefinitely. I moved to the administrative printer at the far end of the corridor — the one the charge nurses used for shift reports, away from the main nursing station. I printed the authorization logs first, then the transfer records, then the time-off documentation with the conflicting timestamps. I organized everything in chronological order as it came off the tray, paper-clipping each section separately. I made two full sets. One for Glen, one to keep somewhere safe outside the hospital. The printer was slow, the kind that pauses between pages long enough to make you anxious, and I kept glancing toward the corridor entrance while I waited. The evidence package, laid out on the counter, was more substantial than I'd expected — nearly forty pages of documentation covering six months of transfers, authorizations, and scheduling records. I tucked both sets into a manila folder I'd brought from home and slid it into my bag. I cleared the printer queue, deleted the print job from the system log, and was reaching for my bag when I heard it — footsteps in the administrative corridor, steady and unhurried, coming closer.
 Image by RM AI
Image by RM AI
Consulting with Glen
I called Glen first thing the next morning and we met at the coffee shop two blocks from the hospital — neutral ground, away from anyone who might recognize us. He looked tired but focused when he sat down across from me, and I slid the manila folder across the table before I'd even taken my coat off. He went through it slowly, page by page, reading the way someone reads a legal document rather than a news article. I walked him through the timestamp conflicts while he cross-referenced the authorization logs against the time-off records I'd pulled. He didn't say much at first. When he got to the conference documentation — the hotel receipt, the registration confirmation, the transfer form bearing my credentials from the same night — he set the page down flat on the table and looked at me over his reading glasses. 'Whoever did this had administrative-level access,' he said. 'This isn't a password someone guessed.' He said the credential mismatches alone carried serious federal implications — wire fraud, potentially healthcare fraud statutes depending on what the product was used for. Then he tapped the destination code at the bottom of one of the transfer forms. The Riverside Drive address. He said we needed to know what was actually at that location before we took this anywhere official. We sat with that for a moment, the folder open between us, both of us understanding that the next step would change things considerably.
 Image by RM AI
Image by RM AI
The Destination Address
I spent that evening searching public records databases — property registrations, business filings, state medical licensing directories. The Riverside Drive address came up quickly enough. Suite 12 was registered as a private medical office under a corporate LLC name that meant nothing to me — a string of initials that didn't correspond to any practice name I recognized. I checked St. Jude's official partner facility directory, the one the hospital published for referral purposes. The address wasn't in it. I checked the regional hospital network's affiliated clinic list. Not there either. I searched the state medical board's licensed facility registry and found a registration, but the listed services were vague — 'private wellness consultations' — and the supervising physician name attached to the license was one I'd never encountered in twenty-five years of working in this system. The building itself, from what I could find in property records, was a high-end professional complex three blocks from St. Jude's — the kind of address that costs serious money per square foot. I cross-checked the LLC against the hospital's vendor and contractor records. Nothing. No contract, no affiliation agreement, no memorandum of understanding. The plasma from our blood bank had been routed, week after week, to a private medical office with no official connection to St. Jude's Hospital whatsoever.
 Image by RM AI
Image by RM AI
The Private Clinic Discovery
I told myself I was just going to walk past. I had a forty-minute lunch break and the building was three blocks away, and I needed to see it with my own eyes rather than through a property record. I found the address without any trouble — a glass-and-steel professional complex set back slightly from the street, the kind of building that announces money without announcing itself. Suite 12 was around the side, accessible through a separate entrance that faced a small landscaped courtyard. There was no signage on the door. No practice name, no hours posted, no logo on the frosted glass panel beside the keycard reader. Just a brushed-metal suite number and a small intercom panel. The entrance itself was immaculate — polished stone threshold, recessed lighting above the door, the kind of finish work that costs more per square foot than most hospital lobbies. While I stood near the courtyard pretending to check my phone, two people came out through that door. Both well-dressed, both moving with the unhurried ease of people who expected their surroundings to be exactly this nice. Neither of them looked like they were leaving a routine appointment. I walked back to the hospital slowly, turning it over in my mind. Whatever was behind that unmarked door, it wasn't a standard medical practice. The quiet luxury of it, the deliberate absence of any public-facing identity, stayed with me the rest of the afternoon.
 Image by RM AI
Image by RM AI
Understanding the Setup
I sat in my car after my shift ended and didn't start the engine for a long time. I laid it out in my head the way I'd been trained to think through a clinical problem — start with what you can observe, work outward from there. Someone had taken my login credentials and used them to authorize transfers over a period of months. The transfers followed a precise schedule. The product ended up at a private, unaffiliated clinic with no public identity and what looked like a wealthy clientele. And my name was on every single authorization form. If anyone pulled those records — a regulator, an auditor, a law enforcement agency — the trail led directly to me. The real movement of product, the real destination, the real people involved — none of that was visible in the paperwork. Only my credentials were. I thought about the timing of Marcus's accusations against me, how quickly the formal complaint had followed, how neat and complete the documentation against me had looked when Rita laid it on the table. I couldn't connect all the pieces yet. I didn't know who had access to my login, or who was behind the clinic, or how far back any of this went. But sitting there in the parking garage with forty pages of evidence in a folder on the passenger seat, the weight of how completely and carefully I'd been set up pressed down on me like something I couldn't lift.
 Image by RM AI
Image by RM AI
Glen's Confirmation
I called Glen the morning after I'd sat in that parking garage and asked if we could meet somewhere that wasn't the hospital. He suggested a diner two miles from the building — a place he'd used before for exactly this kind of conversation, he said. I spread everything out on the table between us: the photos I'd taken of the Riverside Drive building, the transfer logs, the authorization forms with my credentials on them, the address. Glen went quiet in a way that felt different from his usual measured silence. He pulled out his phone and started searching while I watched him work through it. He checked the state medical board's public registry first, then a licensing database he had access to through the union. He typed the clinic name three different ways. Nothing came back. No registration. No affiliation with any hospital network. No oversight body listed anywhere. He set his phone down and looked at the photos again, then back at me. He said the building was operating outside every regulatory framework he could find — no board certification, no state licensing, nothing that would make it a legitimate medical facility by any standard he knew. He said that for a place apparently handling plasma products, that absence wasn't just unusual. It was a serious problem. He tapped the address on the table between us and said we needed to find out who owned this place.
 Image by RM AI
Image by RM AI
The Next Move
We stayed at that diner table for another hour after Glen confirmed what I'd already suspected. He ordered more coffee and I spread the transfer logs out again, and we talked through what we actually had versus what we still needed. What we had was a paper trail connecting my credentials to a facility that had no legal standing as a medical operation. What we didn't have was any name — any person — behind the corporate entity that owned the building. Glen said that in his experience, when something was set up this carefully, the ownership structure was usually the key. Find who owns it, he said, and you find who benefits. He walked me through the public records that would be available — county property filings, state corporate registrations, business entity databases. He said the union had access to some business registration tools that weren't widely known, and he'd work that angle. He told me to start with the county clerk's office, pull the property record for the Riverside Drive address, and document every corporate name that appeared, no matter how generic it looked. He was careful about one thing: he said we needed to stay inside public records only. Nothing that could be challenged later. I agreed. We split the work between us, and before we left, Glen wrote down the exact search sequence I should follow. I folded the paper and put it in my pocket next to the transfer logs.
 Image by RM AI
Image by RM AI
Public Records Search
I used a vacation day I'd been holding onto for months and drove to the county clerk's office on a Tuesday morning when I knew it would be quiet. I brought a notepad, a pen, and the Riverside Drive address written on a card in my pocket. The clerk at the front desk pointed me toward the public terminal and told me property records were searchable by address. I typed in the street number and waited. The record came back quickly enough — the building had changed hands about four years ago. The current owner of record wasn't a person. It was a corporate entity: Riverside Medical Holdings LLC. I wrote that down and asked the clerk if I could request the associated corporate filing documents. She handed me a form and told me it would take about twenty minutes. I sat in a plastic chair near the window and waited. When the documents came back, I spread them on the counter and started reading. The filing listed a registered agent — a law office in the financial district — and a managing member that was listed not as an individual but as another corporate entity entirely. I wrote down every name on every page. The structure wasn't simple. It wasn't meant to be. The property on Riverside Drive was registered to Riverside Medical Holdings LLC — a name that told me nothing about who was actually behind it.
 Image by RM AI
Image by RM AI
Shell Company Layers
I took the corporate name Glen had helped me identify and started pulling the thread. Riverside Medical Holdings LLC was registered to a managing member called Crestline Capital Group. I searched Crestline Capital Group in the state business entity database and found it was itself registered to a third entity — something called Harborview Administrative Services, incorporated in Delaware. Delaware registrations are notoriously thin on detail, and this one was no different. The registered agent was a commercial filing service that handled hundreds of companies. No individual names. No addresses beyond a P.O. box. I printed what I could and kept going. Harborview Administrative Services listed its own managing member as a trust — a numbered trust with no public beneficiary information. I sat back from the terminal and looked at what I'd assembled. Four layers. Each one pointing to the next, each one requiring a separate search in a separate database, each one yielding another corporate name instead of a human being. I'd been doing this for three hours and I was no closer to a person than when I'd started. I knew this kind of structure existed — I'd read about it in the context of financial fraud cases — but seeing it built around what was supposed to be a medical facility made something cold settle in my chest. I gathered my printed pages into a folder and sat with the weight of how thoroughly the trail had been buried.
 Image by RM AI
Image by RM AI
Financial Records
The corporate filings I'd collected didn't have full financial statements, but some of the entities had filed annual reports with the state that included revenue disclosures — basic figures, nothing detailed, but enough to read. I went back through the documents I'd printed and started pulling the numbers. Crestline Capital Group had filed a report two years prior showing gross receipts in the range of four million dollars for that fiscal year. The year before that, the figure was closer to two and a half million. I sat with those numbers for a moment. I'd worked in hospital supply management long enough to know what plasma products cost at wholesale, and I'd done rough calculations based on the transfer volumes I'd documented. Even at a significant markup, simple resale of the diverted product wouldn't come close to generating that kind of revenue. The money flowing through these entities was substantially larger than what the plasma transfers alone could account for. Something else was generating income — something ongoing, something that produced consistent revenue across multiple fiscal years. I didn't know what that was yet. I wrote the figures down next to my transfer volume estimates and drew a line between them, and the gap between those two numbers sat on the page like a question I didn't have an answer to yet. The scale of what was moving through those accounts was larger than anything I'd imagined when I first pulled those transfer logs.
 Image by RM AI
Image by RM AI
Patient Scheduling Data
I almost missed it. I'd been going through the corporate documents for the fourth time when I found a reference I'd skimmed past earlier — a single line in an administrative filing that mentioned a scheduling platform by name, something called ClearPath Client Management. I searched the name and found it was a private appointment software used by boutique medical practices. That detail sat with me. I went back to the plasma transfer logs and laid them out in date order, then pulled up the ClearPath reference again. The filing included a data retention notice that listed appointment volume by quarter — not client names, just aggregate numbers. I matched those quarters against the transfer dates. The correlation was exact. Every quarter that showed a spike in plasma transfer volume also showed a corresponding spike in scheduled appointments. Not approximate. Not close. The same weeks. I went through it three times to make sure I wasn't seeing what I wanted to see. The plasma wasn't sitting in storage somewhere. It was being used on a schedule — a planned, recurring schedule with an entire administrative system built around it. I thought about the revenue figures I'd found, the four-million-dollar gross receipts, and what kind of medical operation could generate that kind of income from a small, unlisted facility. Then I found the client tier designation buried in the ClearPath filing — a field labeled "Premier Access" with an appointment count that suggested a small, exclusive, and very deliberately managed patient list.
 Image by RM AI
Image by RM AI
The Treatment Pattern
I spread everything across my kitchen table that evening — the transfer logs, the corporate filings, the revenue figures, the appointment data — and tried to look at it as a whole rather than as separate pieces. The plasma volumes I'd documented from the hospital transfers matched almost precisely with what would be needed for regular infusion treatments. I knew the math on that from my clinical background: a standard plasma infusion protocol for an ongoing therapy program, administered to a small patient cohort on a recurring schedule, would consume roughly the quantities I was looking at. The appointment frequency in the ClearPath data suggested treatments every few weeks for each client. The revenue figures suggested those clients were paying significantly for the privilege. The facility had no public profile, no insurance billing, no regulatory oversight. Everything about the structure pointed toward a private operation serving a small number of people who wanted medical treatments outside the normal system and had the means to pay for them. I didn't know yet what specific treatments were being offered, or whether they were medically legitimate, or who was authorizing them. But the picture that was forming wasn't simple theft for resale. What I was looking at appeared to be an actual functioning treatment program built around the diverted supply — organized, scheduled, and apparently running across multiple fiscal years. I sat at that table for a long time after I stopped writing, and the quiet of the apartment felt heavier than it had before I'd started putting the pieces together.
 Image by RM AI
Image by RM AI
Credit Card Receipts
The last documents I hadn't fully reviewed were a set of financial transaction records that had been attached as exhibits to one of the Delaware filings — included, I suspected, because a compliance requirement had forced their disclosure. I almost set them aside. I was glad I didn't. The records showed individual credit card transactions processed through one of the shell entities, each one itemized by date and amount. The charges weren't small. The lowest figure on the page was thirty-two hundred dollars. Several were above five thousand. A handful were above eight. The transaction dates lined up with the appointment schedule I'd already mapped. I pulled out my notes on standard hospital plasma product costs and did the arithmetic. Even at a significant premium over wholesale, the plasma itself couldn't account for charges at that level. These weren't product sales. The pricing structure — the per-transaction amounts, the frequency, the consistency — matched what I'd seen quoted for high-end private infusion therapy in the few concierge medicine billing guides I'd come across in my career. Someone was charging premium medical service rates, not commodity prices, and clients were paying without apparent hesitation. I set the transaction records next to the appointment data and the transfer logs, and the three columns of figures lined up in a way that was hard to look away from.
 Image by RM AI
Image by RM AI
Connecting Payments to Treatments
I pulled out a fresh sheet of paper and built the timeline from scratch. On one side I listed every plasma delivery date I'd extracted from the transfer logs — the shipment timestamps, the quantities, the authorization codes. On the other side I listed every high-value credit card transaction from the Delaware filings. Then I drew the lines. Every charge above five thousand dollars fell within a six-hour window of a recorded delivery. The eight-thousand-dollar transactions — the ones that appeared most frequently — each corresponded to a same-day shipment arrival. Not within a day. Not within two days. Within hours. I checked it three times because I didn't trust myself the first two. The pattern held every single time. Whoever was running that clinic wasn't stockpiling product. They were moving it immediately, straight from delivery to treatment room, billing clients at premium rates before the plasma had time to sit in a refrigerator. The operation ran on fresh supply and fast turnover. I sat back and looked at the two columns side by side — delivery dates, payment dates, amounts, timestamps — and the precision of it settled over me like something cold and very heavy.
 Image by RM AI
Image by RM AI
Marcus's Name in the Filings
I went back through the corporate filings one more time, slower now, reading every line instead of scanning for numbers. The shell companies were layered — one entity owned by another, that one registered to a third, each one incorporated in a different state. I'd already mapped the ownership chain on paper, but I hadn't read every signatory block on every document. I started at the bottom of the stack and worked up. The third filing from the end was an incorporation certificate for a Delaware LLC called Meridian Health Partners. The registered agent line was where I stopped. The name printed there was Marcus Brennan. I read it twice. I turned the page. His signature appeared again on the operating agreement, dated fourteen months ago — roughly six weeks after he'd taken the director position at St. Jude's. I set the page down carefully, the way you set something down when your hands aren't entirely steady. I photographed every page that carried his name, then laid the incorporation certificate flat on the table in front of me. His signature sat at the bottom of the page, neat and unhurried, like a man who had no reason to think anyone would ever look.
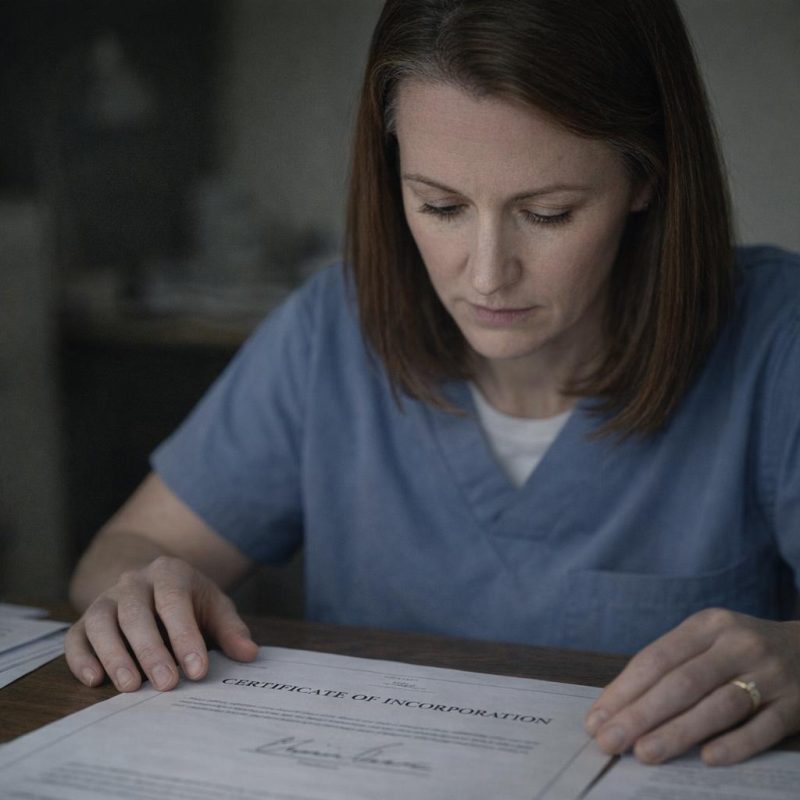 Image by RM AI
Image by RM AI
The Hidden Ownership
I followed the ownership chain the rest of the way. Meridian Health Partners was listed as the managing member of a second LLC, which in turn held a controlling interest in a Nevada holding company called Crestline Medical Properties. I pulled the Nevada registration records I'd downloaded earlier and found the articles of organization. The sole member line listed Crestline Medical Properties. I already had those records. I went back to them and found the property schedule attached as an exhibit — a single commercial address on Riverside Drive. The same address I'd photographed from the street. I cross-referenced the county assessor records I'd pulled two days earlier. The deed listed the owner of the Riverside Drive property as Crestline Medical Properties, LLC. I sat with that for a moment, then kept going. The registered agent for Crestline was a law firm, but the member certificate attached to the operating agreement listed one individual as the sole economic interest holder. I turned to that page and found the name printed there in plain black type — Marcus Brennan, listed as sole owner of the clinic on Riverside Drive.
 Image by RM AI
Image by RM AI
The Systematic Frame-Up
I spread everything out across the kitchen table — the transfer logs, the credential authorization records, the corporate filings, the payment data, the delivery timestamps — and I looked at all of it together for the first time. The authorization codes on every plasma transfer carried my employee ID. My login credentials appeared on each release form, timestamped across a six-month window. I pulled my own shift records and laid them alongside the transfer log. Several of the authorizations were timestamped during hours I was documented as being on a different floor entirely, logged into a separate system for patient charting. My credentials had been used to sign off on transfers I had no access to complete. Someone had my login information and had been using it to move product out of inventory, building a paper trail that pointed directly at me. I went through the dates one by one, matching each transfer to the delivery schedule at the Riverside Drive clinic, and the correspondence was exact. Every transfer fed a delivery. Every delivery fed a billing cycle. And every authorization carried my name. I sat at that table for a long time, the documents arranged in front of me in neat columns, and the full shape of what those records showed was impossible to look away from.
 Image by RM AI
Image by RM AI
The Black-Market Operation Exposed
I understood it all then — completely, without any remaining doubt. Marcus had built a private clinic on Riverside Drive and was selling plasma treatments to wealthy clients at eight thousand dollars a session, marketing what amounted to a black-market longevity therapy to people with money and no questions. To supply it, he'd been diverting hospital plasma from St. Jude's inventory for at least six months. He needed a way to authorize those transfers without triggering immediate flags, so he'd obtained my credentials — my employee ID, my login, my digital signature — and used them to process every single release. My name was on all of it. When the annual audit came around and the inventory shortage surfaced, the paper trail would lead straight to me: twenty-five years of perfect service, suddenly implicated in a systematic theft of controlled medical supplies. I'd be terminated, possibly prosecuted, and too discredited to be believed if I ever tried to explain what I'd found. He'd been running the cost-cutting campaign as cover, building a case that I was a liability, softening the ground so that when the accusation landed it would seem inevitable. The evidence package on my kitchen table documented every piece of it — the ownership chain, the credential theft, the transfers, the payments, the clinic. I picked up my phone and called Glen.
 Image by RM AI
Image by RM AI
Calling Glen with the Truth
Glen picked up on the second ring. I didn't start with pleasantries. I told him I had found the clinic, traced the ownership through four shell companies, and confirmed that Marcus Brennan was the sole owner. I told him about the plasma transfers authorized under my credentials, the payment records, the delivery timestamps, the incorporation documents with his signature. Glen didn't interrupt. When I finished, there was a pause — not the kind that means someone is skeptical, but the kind that means someone is thinking fast. 'How solid is the documentation?' he asked. I told him I had corporate filings, county property records, financial transaction data, transfer logs with timestamped credential use, and shift records proving I wasn't present for several of the authorizations. Another pause. 'Diane,' he said, 'this isn't a labor grievance anymore. This is federal.' He told me not to contact Marcus, not to mention any of this at work, and not to share the documents with anyone at St. Jude's. He said the credential theft alone crossed into federal wire fraud territory, and the plasma diversion would involve the FDA and possibly the DEA depending on how the products were classified. 'We need federal investigators on this immediately,' he said.
 Image by RM AI
Image by RM AI
Compiling the Evidence Package
I started at six in the morning and didn't stop until the light outside had shifted from gray to gold to the flat dark of early evening. I organized everything chronologically first, then by category. Corporate filings in one folder: the Delaware incorporation certificates, the Nevada property records, the operating agreements, every page carrying Marcus's name or signature. Transfer logs in a second folder, each entry cross-referenced to the corresponding delivery timestamp at the Riverside Drive clinic. Financial records in a third: the credit card transaction data, the per-session amounts, the billing frequency. My own shift records in a fourth, with the relevant dates flagged — the ones where my credentials appeared on transfer authorizations during hours I was documented elsewhere in the hospital system. I printed duplicates of everything and made a second complete set. I labeled each document, numbered each page, and wrote a two-page summary that walked through the timeline from Marcus's first week at St. Jude's to the accusation meeting with Rita. Every element connected to the next. Nothing floated loose. By the time I set the last page in place and closed the final folder, the stack on my kitchen table was four inches thick, and every claim in it was supported by a document I hadn't written and couldn't have fabricated.
 Image by RM AI
Image by RM AI
Contacting the Authorities
Glen made the calls the next morning. He reached the state medical board's compliance division first and gave them a summary — the unlicensed private clinic, the diversion of controlled hospital supplies, the credential misuse. They asked him to submit documentation for review and flagged it for priority handling. Then he contacted a federal healthcare fraud unit and walked them through the financial side: the shell company structure, the transaction records, the plasma sales to private clients. They asked for a full evidence review and requested a meeting for the following day. Glen called me after each conversation, relaying what had been said, keeping his voice level and methodical the way he always did when things were serious. I listened, confirmed I had complete copies ready to hand over, and wrote down the meeting time. Then I put on my scrubs, drove to St. Jude's, and worked my shift the same way I had for twenty-five years — checking charts, managing inventory, doing the job. Marcus passed me in the corridor once that afternoon and nodded, the way he always did, unhurried and unbothered. I nodded back and kept walking. That evening I sat at my kitchen table with the evidence folders stacked beside me, and the stillness in the room felt like the moment before something long overdue finally arrives.
 Image by RM AI
Image by RM AI
The Investigators Review
The meeting room Glen had reserved was small and windowless, the kind of space that felt designed for serious conversations. I arrived fifteen minutes early with my evidence folders stacked in order — corporate filings on top, transfer logs beneath, financial records at the bottom — and set them on the table the way I'd laid out medication trays for twenty-five years: methodically, deliberately, nothing out of place. Glen was already there, his worn briefcase open beside him. Agents Torres and Park arrived together, badges clipped, a shared tablet between them. Officers Walsh and Ramos followed two minutes later, Walsh carrying a thick regulatory binder and Ramos with a checklist already in hand. I walked them through everything. The shell company documents. The plasma lot numbers matched against delivery dates. The credential logs showing my employee ID used on shifts I could prove I wasn't working. The financial records tracing payments from private clients back through Marcus's shell companies. Torres asked precise questions. Park cross-referenced dates on the tablet without looking up. Walsh flagged three specific credential violations for the medical board. Ramos confirmed the controlled substance transfers violated state pharmacy law on at least eleven separate counts. It took just over three hours. Nobody rushed. Nobody dismissed anything. At the end, Torres closed the folder in front of her, looked across the table, and said, 'We have enough to move forward.'
 Image by RM AI
Image by RM AI
Marcus Schedules the Final Meeting
The email arrived at 4:47 in the afternoon, routed through the hospital's official HR system with Marcus listed as the sender. The subject line read: Final Resolution Meeting — Mandatory Attendance. The body was clean, corporate, every word chosen to sound procedural and inevitable. He cited the ongoing investigation into inventory discrepancies, referenced the documentation already on file, and noted that the meeting would provide an opportunity to 'resolve this matter efficiently and with minimal disruption to hospital operations.' The meeting was set for nine o'clock the following morning. Rita would be present as HR director. The implication underneath all that careful language was unmistakable — show up, sign the resignation papers, or face termination and a criminal referral. I read it twice, then forwarded it to Glen and to Agent Torres with a single line: 'Tomorrow morning. Nine o'clock.' Glen replied within minutes confirming he'd be there. Torres replied four minutes after that, confirming the team would be in position. I set my phone down on the kitchen table and looked at the email one more time. Marcus had written it expecting a woman with no options left. He had no idea that every word of his careful, confident message was landing in a room that was already set against him — the formal notice of his own undoing, written in his own hand.
 Image by RM AI
Image by RM AI
Walking Into the Final Meeting
I wore my scrubs with the twenty-five-year service badge pinned exactly where it always was. Glen met me in the parking lot at eight forty-five, briefcase in hand, and we walked in together without saying much. The conference room was on the second floor, the same one where Rita had first read me the theft accusations six months ago. Marcus was already seated at the head of the table when we came in, jacket pressed, posture easy, the kind of relaxed that comes from believing you've already won. Rita sat to his left, a folder open in front of her, her expression carefully neutral in the way it always got when she was uncomfortable but following procedure. A set of papers sat near the center of the table — I recognized the format from the last time. Resignation documents. Marcus greeted us with a measured nod and began with formal language about reaching a final resolution, about the weight of the evidence, about the hospital's obligation to act. He spoke the way he always did — smooth, controlled, each sentence landing exactly where he intended it. I sat across from him with my hands folded on the table and let him talk. Glen sat beside me, quiet and still. Somewhere down the hall, in the small office we'd arranged the day before, four investigators were waiting. I already knew how this morning ended. That knowledge sat in my chest, steady and weightless.
 Image by RM AI
Image by RM AI
The Investigators Enter
Marcus was mid-sentence — something about the hospital's legal exposure — when Glen pushed his chair back and stood. He crossed to the conference room door without a word and opened it. Agent Torres came in first, badge displayed, followed by Agent Park, then Officer Walsh and Officer Ramos, all four moving with the unhurried precision of people who had done this before. Torres introduced the team in a single clear sentence: federal agents and state compliance officers, present to conduct an investigation into healthcare fraud, controlled substance diversion, and credential misuse. She named the relevant statutes. Park set a document case on the table. Walsh placed her regulatory binder beside it. Ramos positioned himself near the door. The whole thing took less than ninety seconds. Rita's hand went to her mouth. She looked at Marcus, then at the agents, then back at Marcus, her careful neutral expression completely gone. Marcus had stopped talking the moment the door opened. He sat very still, both hands flat on the table, his eyes moving from Torres to Park to the document case and back again. He asked what was happening. Torres told him they'd get to that. I watched all of it from my seat across the table, hands still folded, back straight. The color had already begun to leave his face.
 Image by RM AI
Image by RM AI
Presenting the Evidence
Torres worked through the evidence the way a surgeon works — no wasted motion, nothing out of sequence. She laid the corporate ownership documents on the table first: the filings for Riverside Medical Associates, Marcus's name listed as sole owner, registered eight months before he took the director position at St. Jude's. Park followed with the transfer logs, each entry timestamped, each plasma lot number cross-referenced against the clinic's treatment schedules. The dates lined up exactly. Walsh set down the credential records next — my employee ID used to authorize transfers on four separate occasions, each one on a day I could be placed elsewhere by time-stamped security footage and shift records. Ramos walked through the pharmacy compliance violations, eleven counts, each one documented with the corresponding transfer entry. Marcus said the documents were taken out of context. Torres didn't argue with him. She just placed the next page on the table. Rita had stopped looking at Marcus somewhere around the third document. She was reading the pages herself now, her glasses pulled down from the chain around her neck, her face going through something I didn't have a clean word for. Glen sat with his hands folded, watching. I sat beside him and watched Marcus look at the evidence of everything he'd built, laid out in order under fluorescent light, each piece fitting cleanly against the next.
 Image by RM AI
Image by RM AI
The Credit Card Trail
Park opened the second document case and began with the credit card records. He laid them out in rows — transaction dates, amounts, client initials, each one printed cleanly on a single page. Eight thousand dollars, paid on the fourteenth. Eight thousand dollars, paid on the twenty-second. The amounts were consistent, the intervals regular, the pattern unmistakable once you saw it laid against the plasma delivery schedule. He placed the treatment appointment logs beside the payment records. The dates matched. Every single one. Then came the bank records — deposits flowing into an account held by a subsidiary of Riverside Medical Associates, the same shell structure Torres had walked through earlier. Marcus had his arms crossed now, jaw set, eyes fixed somewhere past Park's shoulder. He said the payments were for consulting services. Park didn't respond to that. He just placed the next page on the table: a second account, a third, each one receiving transfers from the first, the money moving in a pattern that had no explanation a consulting arrangement could cover. Rita had her glasses off entirely now, pressing them against her palm. Officer Ramos confirmed that each transaction corresponded to a specific treatment appointment and that the payment structure violated medical board financial regulations on its face. Park squared the last page against the others, looked across the table at Marcus, and said, 'Every payment traces directly back to your clinic.'
 Image by RM AI
Image by RM AI
Marcus Confronted
Torres let the silence sit for a moment after Park finished. Then she opened her own folder and began reading. Corporate fraud and embezzlement of controlled substances from a licensed medical facility. Operating an unlicensed medical clinic in violation of state and federal law. Medical malpractice through the administration of unregulated treatments to private clients. Identity theft and fraudulent use of a hospital employee's credentials to authorize the diversion of controlled substances. Grand larceny of hospital property valued at over four hundred thousand dollars across the documented period. She read each charge in the same measured tone, no emphasis, no drama, just the language of the statutes and the facts that supported them. Walsh followed with the state medical board violations — unlicensed facility operation, unauthorized administration of controlled treatments, failure to maintain required oversight documentation. Ramos confirmed the pharmacy law violations aligned with the federal charges. Marcus had stopped responding somewhere around the third charge. He sat with both hands on the table, not moving. Glen was still beside me, quiet. Rita had her folder closed in front of her, both hands pressed flat on top of it, her face unreadable. I watched Torres work through the final items on her list. When she finished, the room was completely still. Marcus's face had gone the color of old concrete, the easy confidence of an hour ago entirely gone from it.
 Image by RM AI
Image by RM AI
The Arrest
Torres nodded to Park, and Park stood and moved around the table. He told Marcus to stand and place his hands behind his back, and he read the Miranda rights in the same even tone Torres had used for the charges — clear, unhurried, each word given its full weight. Marcus stood. He didn't say anything. The handcuffs went on with a sound that was smaller than I expected, a quiet mechanical click in a very still room. Glen put his hand briefly on my shoulder. Rita hadn't moved from her chair. She was staring at the table in front of her, both hands still pressed flat on the folder, and I think she was only beginning to understand the full shape of what had been happening inside the hospital she'd helped run. Walsh told her the state medical board would be in contact regarding the hospital's compliance exposure. Ramos confirmed the clinic would be shut down by end of day. Torres collected the evidence folders from the table with the same methodical care she'd used laying them out. Six months of accusations, suspension notices, and resignation papers, and it was ending in this room, in this quiet, with four investigators and a set of handcuffs. I kept my eyes on the door as Agent Park walked Marcus through it.
 Image by RM AI
Image by RM AI
Terminating the Executive Team
Rita didn't waste any time. While Agent Park was still walking Marcus through the door, she had her phone out and was already dialing the board chair. Glen and I sat in the conference room while she stepped into the hallway, and I could hear the clipped urgency in her voice through the glass — not panic, but the controlled efficiency of someone who understood exactly how bad this looked and how fast it needed to be addressed. Within two hours, an emergency board meeting had been called. Glen walked me through what would happen next, keeping his voice steady and practical the way he always did, and I was grateful for that because my own thoughts kept sliding sideways every time I tried to hold them still. The board reviewed the evidence Torres and Park had laid out — the billing fraud, the ghost clinic, the forged documentation — and the picture it painted of institutional failure was not a small one. By late afternoon, Glen got a call confirming it. Marcus's entire executive team had been terminated, effective immediately, for failure to detect and report the fraud operating under their direct oversight. Rita came back into the room looking like she'd aged five years in an afternoon. She set a printed memo on the table in front of me — the board's formal acknowledgment that my suspension had been issued without cause — and the hospital's internal investigation of all departments had already begun.
 Image by RM AI
Image by RM AI
Clearing My Record
Dr. Calloway met with me in his office two days later. He was silver-haired and composed in the way that board chairs tend to be, but there was something visibly uncomfortable sitting underneath that composure, and he didn't try to hide it. He slid a formal letter across the desk before he said anything else. It was printed on hospital letterhead, signed by the full board, and it stated clearly that all disciplinary actions taken against me had been based on fabricated evidence and were hereby rescinded in their entirety. My personnel file had been expunged. Every suspension notice, every written warning, every accusation — gone, officially and permanently. Rita sat to his left and confirmed that HR had corrected all documentation and that my twenty-five-year service record had been fully restored. Dr. Calloway said he was deeply embarrassed that someone he had hired had used the institution to target a dedicated employee, and that the board accepted full responsibility for the oversight failures that had allowed it to happen. He said it plainly, without hedging, and I respected him for that. I accepted the apology the same way — quietly, without ceremony. I didn't need a speech. I just needed the record to reflect the truth, and now it did. I held the letter in both hands for a moment, and the weight of it — one page, maybe three hundred words — felt like twenty-five years finally settling back into place.
 Image by RM AI
Image by RM AI
The Promotion
Dr. Calloway asked Rita to give us a few minutes, and when the door closed he leaned forward and folded his hands on the desk. He said the board had been discussing the hospital's leadership structure in light of everything that had happened, and that there was a position they wanted to offer me. Chief Director of Clinical Operations — oversight of all clinical departments across St. Jude's, reporting directly to the board. I didn't say anything for a moment. He kept going, telling me that my twenty-five years of service had demonstrated exactly the kind of integrity and institutional knowledge the hospital needed in that role, and that what I had done — documenting the discrepancies, preserving the evidence, holding my ground through six months of pressure — had prevented the fraud from continuing indefinitely. He said the board's view was that I had effectively saved the hospital from itself. I wasn't sure what to do with that. I'd spent the last six months just trying to survive the accusations, and now someone was sitting across from me telling me I'd done something worth honoring. Rita came back in and offered her congratulations with a warmth that felt genuine, and I found I could accept it without reservation. I told Dr. Calloway yes. The word came out steadier than I expected. Twenty-five years of showing up, doing the work, and refusing to cut corners had brought me to this desk, and that felt like the only thing worth saying.
 Image by RM AI
Image by RM AI
Twenty-Five Years Proven
My new office was on the fourth floor, with a window that looked out over the main entrance and the parking structure beyond it. I stood there on my first morning in the role, coffee going cold in my hand, watching the shift change happen below — nurses crossing the lot in their scrubs, a supply truck backing into the loading dock, the ordinary machinery of a hospital morning running exactly as it should. Marcus was facing federal prosecution. The ghost clinic had been permanently shut down. The compliance team had already begun implementing new oversight protocols across every department. And I was standing in an office with my name on the door, twenty-five years of service intact, my record clean. I thought about the morning Rita had called me into that conference room with the accusation letter. I thought about sitting in my car afterward, hands on the steering wheel, trying to figure out how something I hadn't done had managed to look so much like something I had. Six months of that. Six months of suspension notices and union meetings and evidence folders spread across my kitchen table at midnight. I'd kept every document. I'd trusted the process even when the process felt like it was failing me. The truth had been there the whole time — in the billing records, in the timestamps, in the paper trail Marcus had never thought anyone would follow. I pressed my hand flat against the glass and looked out at the hospital I had given my career to, and it looked exactly like what it was: mine to protect.
 Image by RM AI
Image by RM AI
KEEP ON READING

20 Strangest Beauty Trends Throughout History
Beauty Has Always Had Strange Rules. History is full of…
By Christy Chan Jun 12, 2026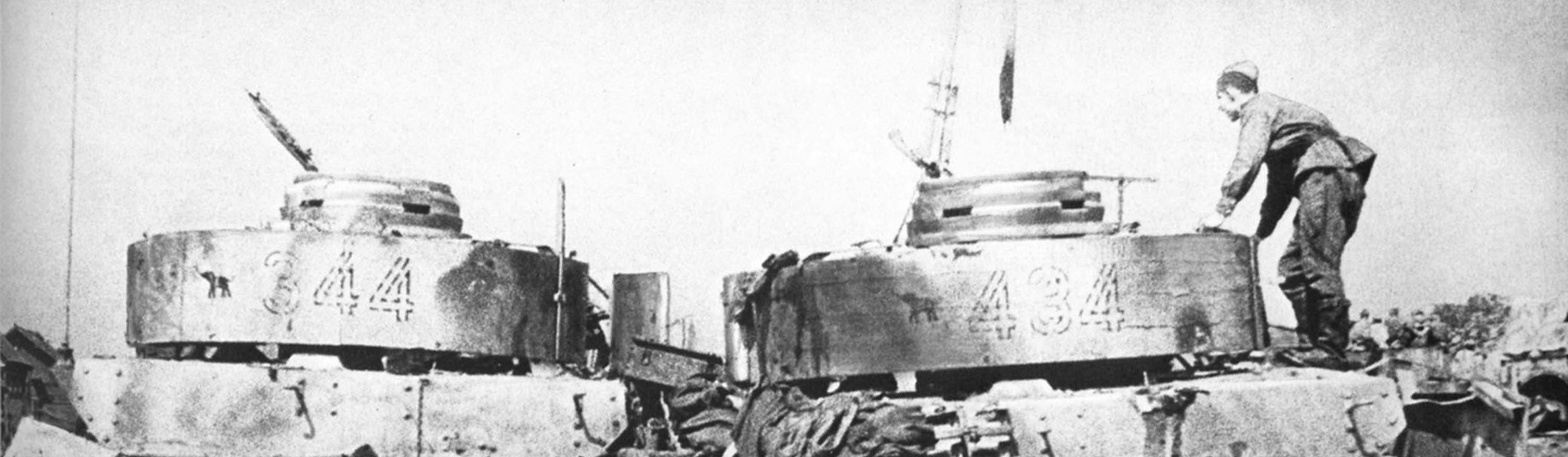
10 Tiny Decisions That Changed History & 10 Tiny Mistakes…
The Small Moments That Moved the World. History gets taught…
By Cameron Dick Jun 10, 2026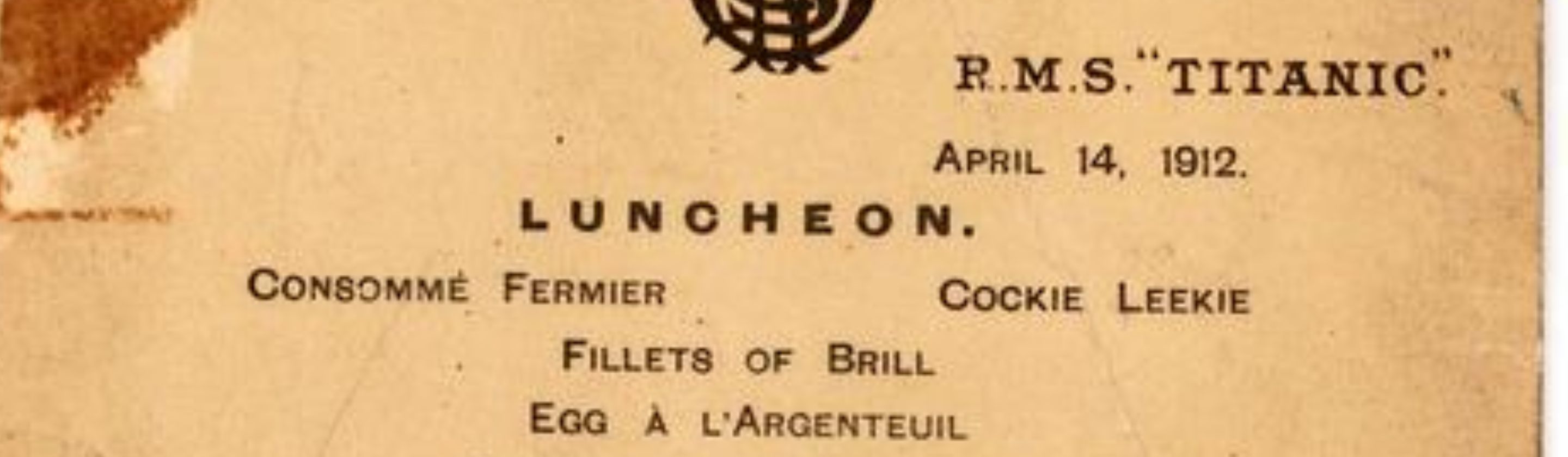
20 First Class Meals Served On The Titanic's Final Night
The Ultimate Final Feast. When the wealthiest passengers gathered in…
By Sara Springsteen Jun 12, 2026
20 Facts About The Library of Alexandria
More Than Just A Room. The Library of Alexandria has…
By Elizabeth Graham Jun 12, 2026
The 20 Creepiest People In History
Truly Uncomfortable. History isn’t only made by kings, reformers, and…
By Annie Byrd Jun 12, 2026
10 Ships That Made History & 10 That Disappeared Without…
Voyages That Changed The Record. Ships have carried explorers, soldiers,…
By Rob Shapiro Jun 9, 2026