
I Stayed with My Sister in the Hospital for a 'Routine Issue'—What I Found in Her Medical Records Made My Blood Run Cold
I Stayed with My Sister in the Hospital for a 'Routine Issue'—What I Found in Her Medical Records Made My Blood Run Cold
The Steady One
I need to tell you about what happened when my sister Carla was admitted to the hospital last November. She'd called me on a Wednesday afternoon, trying to sound casual about it, saying her doctor wanted her to come in for observation. 'Just routine,' she said, like she was scheduling an oil change. But Carla's never been hospitalized before, not in fifty-eight years. When I got to her room that evening, she was sitting up in bed scrolling through her phone, wearing the terrible gown they give everyone. 'You didn't have to come,' she said, which we both knew was a lie. I'm the older sister, and I've looked after her since we were kids—that's just how it works with us. She kept making jokes about the hospital food, about how the IV made her feel like a cyborg, about how she'd finally have time to catch up on her shows. But her hands were doing that thing they do when she's nervous, picking at the blanket edge. The doctor had mentioned some irregularities in her bloodwork, nothing specific, just wanted to monitor her overnight. 'Probably nothing,' Carla said again, and I nodded like I believed her. Something about the way Carla kept reassuring me made me more worried, not less.
 Image by RM AI
Image by RM AI
Routine Procedures
The first few hours felt completely normal, exactly what you'd expect from a hospital stay. A different nurse came in every hour or so to check Carla's vitals, writing numbers on a whiteboard by the door. We watched two episodes of some cooking competition show, and Carla critiqued the contestants' techniques while picking at her dinner tray. Around eight o'clock, a phlebotomist came to draw blood—young guy, probably in his twenties, very efficient. He labeled the vials right there in front of us, which I noticed because my friend Karen always complains about medical errors. Everything seemed fine. Then Nurse Bailey came in to update Carla's chart, and I watched her write something down, pause, and really look at what she'd written. She scratched it out completely, started writing again in the same spot. It wasn't dramatic or anything, just one of those small moments that catches your attention. I almost asked what she'd corrected, but Carla was telling me about her neighbor's new dog, and the moment passed. Nurse Bailey seemed competent, maybe a little tired, checking her watch like she had somewhere else to be. I figured everyone makes minor mistakes on paperwork. Still, I found myself watching the chart more carefully after that. Nurse Bailey wrote something on Carla's chart, then scratched it out and started over.
 Image by RM AI
Image by RM AI
Processing Error
Maybe an hour later, that same phlebotomist from before came back into the room, and I immediately knew something was off. He had that apologetic look on his face before he even spoke. 'I'm so sorry,' he said to Carla, 'but we need to redraw your blood. There was a processing error with the first sample.' Carla groaned but held out her arm again, making some joke about being a human juice box. But I noticed the look that passed between him and Nurse Bailey, who'd appeared in the doorway like she was supervising. It wasn't much, just a quick glance, the kind of silent communication that happens between coworkers when something's gone wrong. The phlebotomist—his badge said Marcus—was extra careful this time, narrating every step like he was being evaluated. He cleaned the site twice, used a fresh needle obviously, labeled the vials while we watched. 'All set,' he said, but his voice was tight. Processing errors happen, I know that. Labs mix up samples, drop test tubes, whatever. It's a hospital, people are overworked. But as Marcus walked toward the door, vials in hand, I watched him stop in the hallway and check each label again. Once. Twice. As he left, I noticed he double-checked the label three times—like he couldn't afford another mistake.
 Image by RM AI
Image by RM AI
The Hallway Conversation
I couldn't sleep that night in the vinyl recliner they call a guest chair, so around two in the morning I went to find coffee. The hallways were that special kind of quiet hospitals get at night, just the beeping of machines and squeaking of nurse shoes. I was standing at the coffee station near the nurses' break room when I heard voices through the door, which was cracked open about six inches. I recognized Nurse Bailey's voice first, then Marcus the lab tech. 'These results don't match her history at all,' one of them said. I froze, my hand on the coffee pot. 'Are we sure it's the same patient?' That was Marcus, I think, sounding confused. 'The system pulled her file automatically, so it should be,' Bailey replied, 'but something's clearly off.' I should have announced myself, cleared my throat, something. Instead I just stood there listening, my heart starting to pound. They were talking about test results, comparing numbers, using medical terms I didn't understand. Then Bailey said something about checking with the attending in the morning, and I heard footsteps coming toward the door. They saw me standing there and immediately changed the subject, but I'd already heard enough.
 Image by RM AI
Image by RM AI
The Chart Request
I waited until morning, until the shift change was over and Carla was awake, before I asked to see her chart. I tried to sound casual about it, like I was just curious, not like I'd spent the rest of the night replaying that overheard conversation in my head. Dr. Chen came in around nine for rounds—professional, polished, the kind of doctor who makes eye contact but keeps moving. 'Of course,' she said when I asked, 'patients have the right to review their records.' But there was something in her tone, maybe a slight hesitation, that made me more determined. She handed me a tablet with Carla's digital chart, showed me how to scroll through it. The first few pages were standard admission forms, vitals logs, nothing interesting. Then consent forms, insurance verification, all the bureaucratic stuff. I kept scrolling, and Dr. Chen kept standing there watching me, which felt odd. Page five, page six, just routine documentation. Then I hit page seven and stopped. There was a document from somewhere called Ridgeway Medical Associates, dated six months ago, detailing a cardiology consultation Carla had supposedly had. My sister was looking at her phone, oblivious. Dr. Chen's expression hadn't changed. Buried on page seven was a document referencing a clinic neither of us had ever heard of.
 Image by RM AI
Image by RM AI
Ridgeway Medical
I read the document three times before saying anything. It described a consultation for an arrhythmia, included test results, even had a treatment recommendation. The patient name was definitely Carla's, along with her date of birth and our mother's maiden name for verification. 'Carla,' I said, keeping my voice level, 'have you ever been to Ridgeway Medical Associates?' She looked up from her phone, confused. 'Ridgeway what? Never heard of it.' I turned the tablet toward her. 'It says you had a cardiology appointment there in May.' Her face went pale as she read it. 'That's not possible. I've never had heart problems. I've never even seen a cardiologist.' I pointed at the date—May 14th. 'Where were you in May?' Carla's hand went to her mouth. 'I was with you,' she said slowly. 'We were in Charleston for Mom's birthday. The whole week.' I remembered. We'd rented that house on the beach, spent five days there. Carla had been with me every single day. 'This makes no sense,' she whispered, scrolling through the document. The diagnosis listed was dated six months ago—during a time when Carla was on vacation with me.
 Image by RM AI
Image by RM AI
The Rehearsed Answer
Dr. Chen came back an hour later, and I was ready for her. 'We need to talk about this Ridgeway Medical document,' I said, showing her the tablet before she could start her usual routine. She glanced at it, and something flickered across her face—recognition, maybe discomfort. 'Ah, yes,' she said, and what followed sounded like she'd practiced it. 'Sometimes records get shared between systems when facilities are part of the same network. There can be integration issues where documents appear in the wrong patient file. It's a known issue with the software we use.' Her explanation was smooth, technical enough to sound credible, but delivered with the kind of careful precision that made me think she'd given it before. 'But this isn't just appearing in the wrong file,' I said. 'It has my sister's name on it. Her birth date. Everything.' Dr. Chen nodded sympathetically. 'I understand your concern. The system sometimes auto-populates fields incorrectly during transfers. I'll submit a correction request to medical records.' She was already backing toward the door, ready to move on to her next patient. 'How long will that take?' I asked. 'These things can take a few days to process,' she said. She wouldn't look directly at me when she said it.
 Image by RM AI
Image by RM AI
Looking Into It
After Dr. Chen left, I went straight to the nurses' station. Nurse Bailey was there, typing something into a computer, and she looked up when I approached. I explained the situation as calmly as I could—the Ridgeway document, the impossible date, Dr. Chen's explanation that didn't quite add up. Bailey listened, nodding along, her face carefully neutral. 'We're looking into it,' she said when I finished. Just that. Looking into it. 'What does that mean exactly?' I asked. 'Who's looking into it? When will we have answers?' She gave me that sympathetic smile healthcare workers perfect, the one that's meant to be reassuring but just feels dismissive. 'Medical records issues go through a specific department. Dr. Chen filed the request, and they'll investigate the discrepancy. It's standard protocol for this kind of thing.' I wanted to push harder, to demand more specific answers, but what was I going to do? I'm not a doctor. I don't understand their systems. Carla was still admitted, still under their care. So I thanked Bailey and went back to the room, where I tried and failed to sleep in that awful chair, the fluorescent lights humming above me. I kept thinking about those two words—looking into it—and wondering what they were actually doing.
 Image by RM AI
Image by RM AI
The Wrong Chart
The next morning, a doctor I'd never seen before walked into Carla's room with a tablet in his hand and a serious expression on his face. Dr. Rodriguez, his badge said. He introduced himself, then launched into questions that made absolutely no sense. He asked Carla about chronic migraines she'd supposedly reported at intake. She looked at him, confused. 'I don't get migraines,' she said. He frowned at his tablet, scrolled, asked about a family history of autoimmune disorders. 'Not that I know of,' Carla said, glancing at me. He kept going—previous surgeries she hadn't had, medications she'd never taken, symptoms she'd never experienced. Each question made Carla's voice smaller, more uncertain. I stood up. 'I think there's been a mistake,' I said. 'Those aren't her symptoms.' Dr. Rodriguez looked at me with that patient expression doctors use when family members interrupt, then turned back to Carla. 'According to your chart, you've had recurrent episodes of vertigo and balance issues for several years.' Carla's face went pale. 'I haven't,' she said. 'I've never had any of that.' She looked genuinely frightened now, like she was being gaslit in real time. When Carla said 'I think you have the wrong chart,' the doctor just frowned at his tablet and said, 'This is the information we have on file.'
 Image by RM AI
Image by RM AI
The Full Copy
I'd had enough. I marched straight to the nurses' station and told Nurse Bailey I wanted a full copy of Carla's medical records. Every page. Every form. Everything they had. Bailey hesitated, gave me some speech about privacy protocols and administrative processing times. 'I'm on her HIPAA authorization,' I said. 'I want the records today.' She made a phone call. Then another. Someone from medical records came up, explained it would take time to compile everything, that I'd need to fill out a formal request. I stayed right there at that desk, arms crossed, and told them I'd wait. You know what? It's amazing how quickly things move when you refuse to leave. An hour later, they handed me a manila envelope. I went back to Carla's room and opened it. The stack of papers inside was thick—discharge summaries, intake forms, nursing notes, lab results, consultation reports. I started flipping through, trying to organize it chronologically, and that's when I realized something was seriously wrong. There were too many pages. Duplicate sections. References to visits Carla had never made. I spread everything out on the little rolling table, trying to make sense of the timeline. The stack of papers they handed me was twice as thick as it should have been.
 Image by RM AI
Image by RM AI
Piece by Piece
I took the records down to the hospital cafeteria because I couldn't think straight in that room with all the beeping machines and Carla sleeping fitfully. I bought terrible coffee and found a corner table, then started going through everything page by page. The Ridgeway referral form was in there, dated wrong as we already knew. But as I kept reading, I found other things that didn't match. A cardiology consultation from two years ago that mentioned a patient named Carla Thornton—close, but Carla's last name is Thornhill. An allergy notation for shellfish when Carla eats shrimp constantly. A note about a previous hospitalization in Denver, but Carla's never even been to Colorado. I pulled out my phone and started taking notes, documenting every discrepancy. Then I found an intake form from another admission—same hospital, but six months ago. The name was Carla M. Thornton. Patient address was in the same zip code as Carla's. Same insurance provider. And then I saw it, right there in the patient demographics section: the birthdate was off by three digits—April 15, 1964 instead of April 12, 1965.
 Image by RM AI
Image by RM AI
The Merger
I sat there staring at that date, and suddenly everything clicked into horrible focus. This wasn't just a mix-up with one document. Someone—some system, some person, some process—had merged two different patients' files. Carla Thornhill and Carla Thornton. Similar names, similar ages, same insurance company, same general area. And somehow their medical histories had gotten tangled together in the hospital's records. I started separating the papers into two piles, trying to figure out what belonged to my sister and what belonged to this other woman. The actual Ridgeway form belonged to Thornton. So did the migraines, the vertigo, the autoimmune history Dr. Rodriguez had asked about this morning. All of it was someone else's medical reality being imposed on Carla. My hands felt cold as I worked through the stack. How long had this been going on? Since her admission three days ago? Since that previous visit six months back? I thought about Dr. Chen making treatment decisions, nurses administering medications, everyone operating off information that was partially fiction. Someone had made decisions about my sister's care based on another person's medical history.
 Image by RM AI
Image by RM AI
Recent Additions
But here's what really got me—what made my stomach drop. The most recent notes in the file weren't from days ago. They were from yesterday. After I'd raised concerns about the Ridgeway document. After Dr. Chen said they were 'looking into it.' Someone had added new entries that referenced the incorrect diagnosis as if it were confirmed fact. A consulting neurologist's assessment mentioned 'chronic vestibular dysfunction consistent with patient history.' There were recommendations for additional testing—an MRI, specialized balance assessments, possibly a referral to an ENT specialist. None of it relevant to Carla's actual condition. I photographed those pages with my phone, my hands shaking so badly I had to steady my wrist with my other hand. At the bottom of one note, I found a treatment plan dated for next week. Scheduled procedures. Specific appointments. A whole cascade of medical intervention Carla didn't need, addressing problems she didn't have, all because someone had failed to catch this merge and then—even after I flagged it—kept building on the faulty foundation. My hands started to shake as I read the treatment plan—procedures scheduled for next week.
 Image by RM AI
Image by RM AI
The Confrontation
I went straight back upstairs with those records and found Dr. Chen in the hallway. I didn't ask politely this time. I told her we needed to talk immediately, and I spread the papers out on the counter at the nurses' station. I showed her the two different birthdates. The two different names. The duplicate entries. The notes about symptoms Carla had never reported. The scheduled procedures for conditions she didn't have. Dr. Chen's face changed as I walked her through it—the professional mask slipping into something that looked like genuine alarm. 'This shouldn't be possible,' she said, which, you know, wasn't exactly reassuring given that it clearly was possible and had actually happened. She picked up the phone and made a call. Then another. Within fifteen minutes, there were three people crowded around that nurses' station: Dr. Chen, a woman who introduced herself as the medical records supervisor, and another administrator whose title I didn't catch. They spoke in these careful, measured tones—the kind people use when they're trying very hard not to say something that could be used against them later. Dr. Chen called in a supervisor, then another, and suddenly three people were in the room speaking in careful, controlled tones.
 Image by RM AI
Image by RM AI
Correcting the Issue
The supervisor—her name was Margaret, gray hair pulled back severely, the kind of woman who probably ran the whole floor—took charge immediately. She apologized. Multiple times. Used phrases like 'deeply concerning' and 'unacceptable error' and 'immediate corrective action.' She assured me they would rectify Carla's records right away, cancel any scheduled procedures, flag the file to prevent future confusion. Dr. Chen stood there looking uncomfortable while Margaret explained their protocols for reporting incidents like this. They made it sound contained. Manageable. A regrettable but isolated mistake. Margaret promised they'd conduct a full review, that patient safety was their top priority, that they took this very seriously. All the right words. And you know what? Part of me felt vindicated. They were finally acknowledging what I'd been saying all along. They were taking action. Carla would be okay. But even as Margaret talked, even as they made their promises and documented their corrections, I kept thinking about Dr. Rodriguez that morning, asking questions from a chart that was fundamentally wrong. About the treatment plan that had been building while they claimed to be investigating. But I kept thinking—if I hadn't been here, if I hadn't asked—would anyone have noticed?
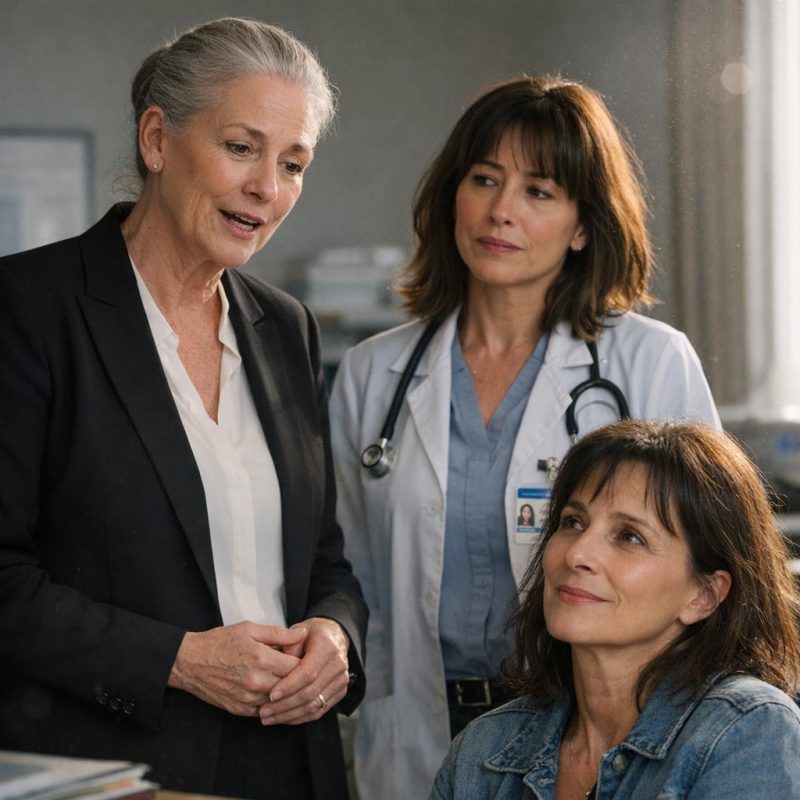 Image by RM AI
Image by RM AI
Not the First Time
Margaret walked me back toward Carla's room, still in full damage-control mode, and then she did something I wasn't expecting. She stopped in the hallway, glanced around to make sure no one was within earshot, and lowered her voice. 'Ms. Thornhill,' she said, 'I want you to know we're taking this seriously. This kind of error...' She paused, choosing her words carefully. 'We've had issues with the new digital records system. Integration problems. The hospital switched platforms eight months ago, and there have been some complications with how patient data migrates and merges.' I stared at her. 'You're saying this has happened before?' She hesitated just long enough that I knew the answer before she said it. 'We've identified a few cases where similar names or demographics caused the system to incorrectly link records. We're working with the vendor to resolve the underlying technical issues.' A few cases. Not one mistake. Not an isolated incident. A pattern. A known problem. When I asked how many patients had been affected, she didn't answer right away—and in that silence, I understood.
 Image by RM AI
Image by RM AI
The New System
Margaret explained the system like she was walking me through something routine, almost mundane. The hospital had transitioned to a new digital records platform eight months earlier—one of those big enterprise systems designed to streamline everything, reduce paperwork, improve efficiency. The old system required manual entry and verification at every step, which was slow but, apparently, not profitable enough. This new one used algorithms to automatically merge patient files when it detected partial matches in names, birthdates, demographics. 'It's supposed to catch duplicate records,' Margaret said, her voice careful and measured. 'If someone's been treated at multiple locations within the network, the system consolidates their information so providers have a complete picture.' It sounded reasonable when she explained it that way. Efficient, even. But then she added, almost as an afterthought, that the matching parameters were 'somewhat broad' to avoid missing legitimate duplicates. I asked what 'somewhat broad' meant. She hesitated. 'The system will merge records if there's a seventy percent match in identifying factors. Names with similar spellings, birthdates within a few days, addresses in the same zip code.' Seventy percent. Not one hundred. Not even ninety. I stared at her, feeling something cold settle in my chest. She called it a 'dangerous loophole,' but her tone—careful, practiced, like she'd said this before—suggested it was something worse.
 Image by RM AI
Image by RM AI
The Records Clerk
I asked Margaret if I could speak with someone from the records department directly, just to understand how this had happened with Carla's file. She looked uncomfortable but agreed, making a quick call before leading me down a hallway to a small office tucked behind the nurses' station. That's where I met Jamie, a young clerk with wire-rimmed glasses and the kind of nervous energy that comes from working in a place where mistakes have consequences. He listened as I explained what had happened—the merged records, the mislabeled test results, the treatment plan for a condition my sister didn't have. His face went pale. 'I'm really sorry that happened,' he said, his voice quiet. 'The system... it's been problematic.' I asked him what he meant by problematic. He glanced toward the door, then back at me, his hands fidgeting with a pen on his desk. 'I'd need authorization to discuss specific cases or system issues,' he said carefully. 'There are protocols.' But the way he said it—the way he looked at me, like he was trying to communicate something he couldn't say out loud—told me everything I needed to know. He wanted to talk. He just couldn't. I gave him my phone number and asked him to call me if he ever felt he could. He took the paper and nodded, but he didn't promise anything. He said he couldn't talk about it without authorization, but the way he looked at me suggested he wanted to.
 Image by RM AI
Image by RM AI
The Discharge Papers
Two days later, Dr. Chen came in with Carla's discharge papers and a smile that was supposed to be reassuring. 'Everything's been corrected in the system,' she said, handing me a printed summary of Carla's actual medical history—clean, accurate, no mention of chronic kidney disease or the medications they'd almost started her on. 'The original issue was minor, just as we thought. Some inflammation, likely stress-related. Rest and hydration, and she should be fine.' Carla looked relieved, almost giddy. She was ready to go home, to put the whole nightmare behind her. Dr. Chen went over the discharge instructions—follow up with her regular doctor in two weeks, call if symptoms worsened, the usual. She was professional, apologetic even, but there was something perfunctory about it all. Like we were checking boxes. I wanted to ask more questions—how exactly had the records been merged, who had access to the system, what safeguards were supposed to prevent this—but Carla just wanted to leave. She was signing papers, gathering her things, thanking the nurses. And I stood there, holding the corrected records, trying to reconcile the relief on my sister's face with the knot of unease still sitting heavy in my stomach. As we packed up, I couldn't shake the feeling we'd been lucky—that we'd narrowly avoided something neither of us fully understood.
 Image by RM AI
Image by RM AI
Walking Out
We walked out through the main lobby, past the reception desk and the rows of plastic chairs in the waiting area. Carla was chatting about what she wanted to eat when we got home, already moving on, already forgetting. But I kept thinking about Margaret's carefully chosen words, about Jamie's nervous glance toward the door, about the phrase 'a few cases' and what it really meant. How many was a few? How many patients had walked through these same doors, trusting the people in white coats and the machines that beeped and whirred, not knowing their records were wrong? How many had been less lucky than Carla—had actually received the wrong treatment, the wrong medication, because some algorithm decided they were seventy percent similar to someone else? I held the door for Carla as we stepped out into the afternoon sunlight, the hospital looming behind us like something solid and permanent. From the outside, it looked the same as it always had—clean, modern, professional. But I knew now what could happen inside, behind the polite explanations and routine procedures. I turned back to look at the building and wondered how many other patients were walking around with the wrong information in their files.
 Image by RM AI
Image by RM AI
Carla's Relief
At home, Carla curled up on the couch with a cup of tea and the kind of relief that comes from narrowly avoiding disaster. She wanted to rest, to watch something mindless on TV, to forget the hospital had ever happened. I understood that impulse—God knows, I did. But I couldn't stop thinking about the other patients Margaret had mentioned. The 'few cases' where the system had done the exact same thing. Those people had names, lives, families who loved them. And if we hadn't caught the error when we did, if I hadn't been there to notice the discrepancy, Carla could have been one of them. That night, I brought it up carefully. 'I think we should report what happened,' I said. 'Not just to the hospital, but to someone outside. The state health department, maybe, or—' Carla's face fell. She set down her tea and looked at me like I'd suggested burning the house down. 'Evie, please,' she said quietly. 'It's over. They fixed it. I just... I just want to move on.' I could see the exhaustion in her eyes, the way her shoulders sagged. She'd been through enough. But somewhere in the back of my mind, I kept hearing Margaret's voice: 'We've identified a few cases.' When I suggested we should report what happened, Carla's face fell—she just wanted it to be over.
 Image by RM AI
Image by RM AI
The Patient Advocate
The next morning, I called the hospital's patient advocacy line. I didn't tell Carla. A woman named Rachel answered, her voice warm and professional in that practiced way that makes you think everything's under control. I explained what had happened—the merged records, the incorrect diagnosis, the treatment that had almost been started. She listened without interrupting, making small sympathetic sounds at the appropriate moments. 'I'm so glad your sister is okay,' she said when I finished. 'And I want to assure you, we take these matters very seriously. There will be an internal review of the incident.' I asked what that meant, exactly. What would the review involve? Who would see it? She gave me vague reassurances about 'quality assurance processes' and 'system audits,' but nothing concrete. Nothing that suggested actual accountability. I pressed harder. 'How many other patients has this happened to?' There was a pause. 'I'm not at liberty to discuss other cases,' she said carefully. 'But I can tell you that patient safety is our top priority.' It was the kind of answer that said everything and nothing at the same time. I thanked her and was about to hang up when she said something that stopped me cold. Her voice dropped, just slightly. 'Ms. Thornhill? Be careful who you talk to about this.'
 Image by RM AI
Image by RM AI
The Research Begins
That warning rattled around in my head for the rest of the day. Be careful who you talk to. What did that mean? Was it a threat? A genuine concern? I didn't know, but it made me start digging. I pulled out my laptop and started searching—hospital name, medical records errors, wrong diagnosis. At first, I found the usual stuff: articles about the importance of verifying patient information, statistics about medical errors in general. But then I started looking at patient forums, the kind of places where people share stories the official channels don't want to hear. And that's when things got interesting. There were posts from people describing experiences eerily similar to Carla's. A woman whose records were merged with someone who had diabetes—she was nearly given insulin. A man who was scheduled for cardiac surgery he didn't need because his file was mixed with another patient's. The details varied, but the pattern was the same: automatic system merges, incorrect information, near-misses with serious consequences. And several of them mentioned the same hospital network Carla had been in. I kept scrolling, my heart pounding harder with each new story. One post, from just three weeks ago, ended with: 'They tried to operate on me for something I never had.'
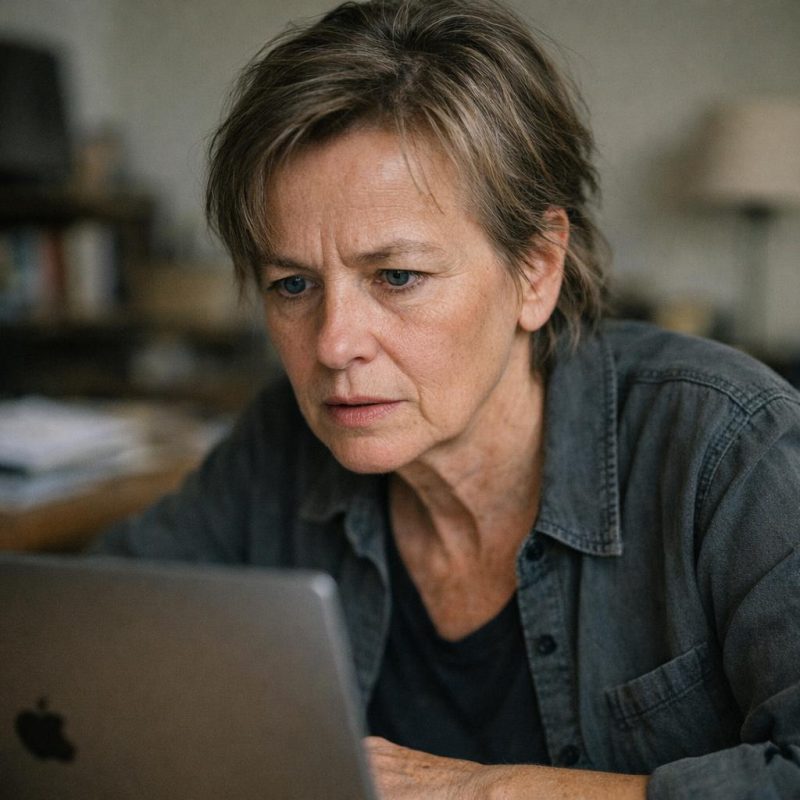 Image by RM AI
Image by RM AI
The Surgery That Wasn't Needed
I clicked on that post and read the whole thing twice. The woman's name was Susan, and she'd gone in for what she thought was a routine gallbladder removal. Simple, straightforward. But when she was being prepped for surgery, she'd overheard the surgical team discussing her 'extensive cardiac history' and planning for additional complications. She didn't have a cardiac history. She'd never had heart problems in her life. She'd demanded to see her records right there in the pre-op room, and that's when they discovered the error—her file had been merged with another Susan, same last name, same insurance provider, birthday two days apart. They'd cancelled the surgery, apologized profusely, assured her it was a one-time glitch. But here's what got me: Susan had requested copies of her records a week later, just to document what had happened. And according to her post, they'd been corrected—completely cleaned up, like the merged information had never existed. No trace of the error. She'd also noticed that the other Susan, the one whose cardiac history had been added to her file, had excellent insurance coverage. She'd looked into it and found that the planned surgery—the one she didn't need—would have been billed at over forty thousand dollars. The woman wrote: 'I asked for my records afterward and they'd been corrected—like the error never existed.'
 Image by RM AI
Image by RM AI
The Insurance Angle
After reading Susan's post, I started scrolling through the forum more carefully. I wasn't just looking for stories about merged records anymore—I was looking for patterns. And honestly? They were everywhere once I knew what to look for. A woman named Patricia posted about being billed for cardiac monitoring she never consented to. A man called Derek wrote about charges for diabetes management when he'd gone in for a sports injury. Another woman, Jennifer, had been billed for pulmonary function tests during what was supposed to be a routine physical. The common thread? All of them had insurance. Good insurance. The kind that would cover expensive procedures without much pushback. Patricia mentioned her bill came to twelve thousand dollars. Derek's was nine. Jennifer's was fifteen, and she'd fought it for six months before her insurance just paid it to make the problem go away. I sat there staring at my laptop screen, this cold feeling spreading through my chest. These weren't just administrative mistakes. These were expensive mistakes. Convenient mistakes. I thought about Carla's stay, about all those tests Dr. Okonkwo had ordered based on her 'history' from Ridgeway Medical. Tests I'd watched them perform. Tests we'd never questioned because we'd trusted they were necessary. I pulled out the itemized bill from Carla's stay and started looking for charges I didn't recognize.
 Image by RM AI
Image by RM AI
The Extra Charges
The bill was twelve pages long. I'd glanced at it when it first arrived, seen the insurance adjustment, figured we'd owe maybe a few hundred dollars in co-pays. But now I went through it line by line with a pen in my hand. Chest CT scan with contrast: twenty-eight hundred dollars. Cardiac enzyme panel: four hundred fifty. Extended metabolic panel: three hundred twenty. Pulmonary consultation: six hundred. Every single one of these charges traced back to tests ordered because of her supposed respiratory issues—the issues from the Ridgeway Medical records, the issues she didn't actually have. I called Carla and read the charges to her over the phone. 'Wait,' she said. 'I don't remember having a CT scan.' 'You did. Tuesday morning, remember? They said it was precautionary.' 'But nobody explained why. I thought it was just part of the workup.' Neither of us had questioned it at the time. Why would we? When a doctor orders a test, you assume there's a good reason. You assume they're looking out for you. The insurance had covered most of it, but our portion still came to just over eight hundred dollars. The total came to over eight thousand dollars—most of it for procedures related to a condition she didn't have.
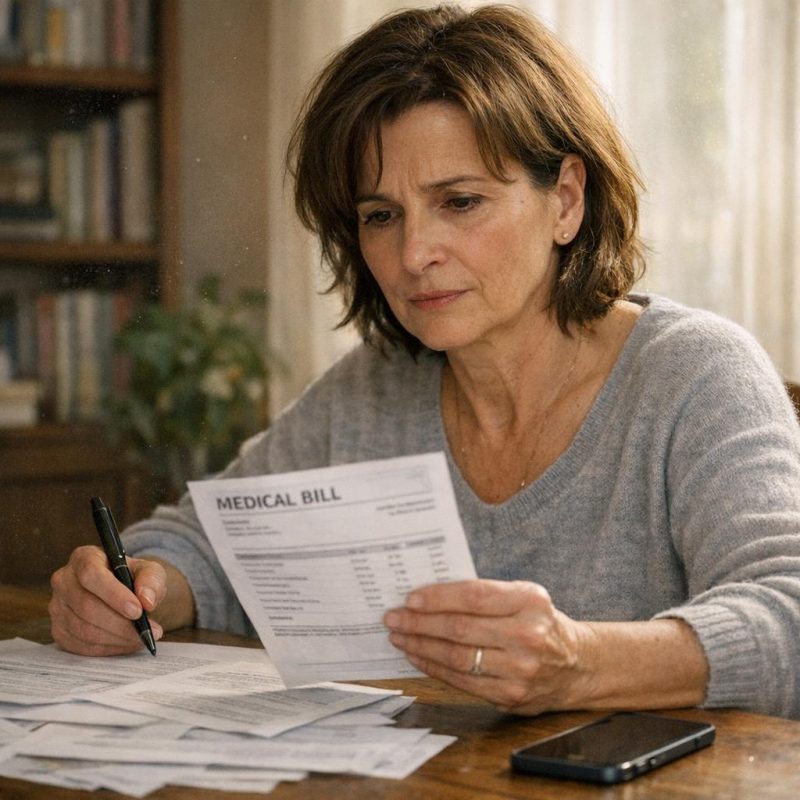 Image by RM AI
Image by RM AI
Disputing the Bill
I called the hospital billing department the next morning. The woman who answered sounded bored, like she fielded calls like this a hundred times a day. I explained the situation calmly—the merged records, the incorrect medical history, the tests ordered based on false information. She asked for Carla's account number and put me on hold. Muzak played for three minutes. When she came back, her tone hadn't changed at all. 'I'm showing all tests were medically necessary based on the patient's history,' she said. 'But the patient history was wrong,' I said. 'That's what I'm trying to explain. The records were merged with someone else's. The respiratory issues weren't hers.' Another hold. This time I waited almost five minutes, listening to some instrumental version of a song I couldn't quite place. I could feel my jaw clenching. When she finally came back on the line, she sounded like she was reading from a script. 'The ordering physician documented medical necessity for all procedures. If you'd like to dispute the charges, you'll need to submit a formal written appeal with supporting documentation.' 'I have documentation,' I said. 'The hospital admitted the records were merged incorrectly.' When I said the patient history was wrong, she put me on hold for ten minutes before coming back with 'I'll escalate this to our review department.'
 Image by RM AI
Image by RM AI
The IT Director
Getting a meeting with Kumar took persistence. I called the IT department four times over two days before someone finally agreed to pass along my request. When he called me back, he sounded cautious, like he was already regretting picking up the phone. But I kept my tone reasonable, framed it as wanting to understand the system better, and he agreed to meet me in his office on Thursday afternoon. Kumar's office was in the administrative building, third floor, tucked away at the end of a quiet hallway. He was younger than I'd expected, maybe late thirties, with dark-rimmed glasses and the slightly rumpled look of someone who spent too much time staring at screens. He shook my hand, gestured to a chair across from his desk. I asked him about the records system, how it worked, how the merging happened. He relaxed a little once he realized I was asking technical questions instead of yelling at him. He explained the digital platform, the centralized database, the way it was supposed to streamline patient care across facilities. 'The algorithm is sophisticated,' he said. 'It uses multiple data points to identify potential matches—name, date of birth, insurance information, that kind of thing. But like any learning system, it has a learning curve.' He described the algorithm as 'sophisticated' but admitted it had 'learning curve issues'—then looked uncomfortable when I asked how often it made mistakes.
 Image by RM AI
Image by RM AI
The Algorithm
I leaned forward in my chair. 'So how does it decide when two records should be merged? What are the thresholds?' Kumar shifted in his seat, his fingers tapping lightly on the edge of his desk. 'It's a weighted scoring system. Name similarity gets a certain number of points, birthdate proximity gets points, insurance match gets points. When the total score crosses a threshold, it flags the records as potential duplicates and prompts a review.' 'Who does the review?' I asked. 'Initially, it's automated. If the score is high enough, the system merges them automatically. Lower scores get flagged for manual review.' 'And what's the threshold for automatic merging?' He hesitated. 'That's proprietary information. It's part of the vendor's algorithm.' I kept my voice calm. 'But someone at this hospital can adjust those thresholds, right? Someone has administrative access?' His jaw tightened slightly. 'In theory, yes. But those settings are locked down. Only certain personnel have that level of access, and all changes are logged.' 'Could someone manipulate those thresholds? Make the system more likely to merge records that shouldn't be merged?' Kumar stood up abruptly, his chair rolling back slightly. 'I think we're done here,' he said. When I asked if it was possible to manipulate those thresholds, he stood up and said our meeting was over.
 Image by RM AI
Image by RM AI
The Follow-Up Call
I drove home feeling like I'd touched something raw, something people didn't want exposed. Kumar's reaction had been too defensive, too quick. If the system was working as intended, why shut down the conversation? That night, around eight-thirty, my phone rang. Unknown number. I almost didn't answer. 'Ms. Hawthorne?' The voice was male, youngish, and tense. It took me a second to place it. 'This is Jamie. From the records department? We met a couple weeks ago.' 'I remember,' I said. 'Is everything okay?' 'I can't talk long. I'm calling from my cell, not the hospital line.' He was speaking quickly, his words tumbling over each other. 'I heard you met with Kumar today. Word travels fast around here. Look, I don't know what you're trying to do, but you need to be careful. This isn't just a records problem. It's bigger than that.' My pulse quickened. 'What do you mean?' 'I can't explain over the phone. Too risky. But if you want to know what's really going on, I can show you. Not here, though. Somewhere else.' 'Where?' I asked. 'There's a coffee shop on Fifth Street, the one near the park. Tomorrow, ten a.m.? Can you meet me there?' He said, 'Meet me tomorrow at the coffee shop on Fifth Street—I can't talk here.'
 Image by RM AI
Image by RM AI
The Coffee Shop Meeting
The coffee shop was small, the kind of place with mismatched furniture and indie music playing too quietly in the background. Jamie was already there when I arrived, sitting at a corner table with his back to the wall. He looked nervous, his eyes darting toward the door every few seconds. I ordered a coffee and joined him. 'Thank you for meeting me,' he said quietly. 'I wasn't sure you'd come.' 'You said you could show me what's really going on.' He nodded, glanced around the shop again. There were only a handful of other people there, none of them paying attention to us. 'I've worked in medical records for six years,' he said. 'I've seen mistakes before—everyone does. But over the past year, it's been different. The merges are happening more often, and they're not random. I've seen dozens of cases like your sister's. Dozens. Records getting mixed up, patients getting tests they don't need, bills going through the roof.' 'Have other people noticed?' I asked. 'Yes. Several staff members have raised concerns. Some of us went to our supervisor. He told us the system was new and we needed to give it time. When we pushed back, he said we were being resistant to innovation. One woman filed a formal complaint with HR. She was let go two months later.' He slid a USB drive across the table and said, 'These are copies—don't tell anyone where you got them.'
 Image by RM AI
Image by RM AI
The Files
I didn't open the files until I got home. I locked the front door, closed the blinds, plugged the USB drive into my laptop like I was handling evidence at a crime scene. There were twenty-three folders on the drive, each one labeled with a patient identification number. I started opening them one by one. The first was a man named Thomas Rivera. His records had been merged with another Thomas Rivera—different middle name, different date of birth, same insurance provider. He'd been billed for cardiology consultations and stress tests based on a heart condition he didn't have. Total charges: eleven thousand dollars. The second was a woman named Linda Chen. Her records merged with another Linda, birthdays eleven days apart. She'd been treated for diabetes complications during a routine wellness visit. Charges: nine thousand. I kept going. Margaret, Sandra, Robert, William. Every single case followed the same pattern. Merged records. Incorrect diagnoses. Expensive tests. Insurance billed. Some patients had disputed the charges. Most hadn't—they'd just trusted the system, paid their co-pays, moved on. By the time I reached the end of the files, my hands were shaking. These weren't random errors. The merges kept happening to patients with good insurance, kept resulting in high-cost procedures. But what made my blood run cold was seeing how many of the 'errors' followed similar patterns—almost like they were designed.
 Image by RM AI
Image by RM AI
The Hospital Administrator
I called the hospital's administrative offices the next morning and scheduled a meeting with Sandra Whitmore, the hospital administrator. I brought printed copies of everything—the merged records, the billing discrepancies, the patterns I'd documented. Her office was on the executive floor, all polished wood and abstract art that probably cost more than my car. She greeted me with a firm handshake and a professional smile, gestured to a leather chair across from her desk. I laid out the evidence methodically, walking her through each case, showing her the patterns. She listened with her hands folded on the desk, nodding occasionally, taking notes on a legal pad. When I finished, she looked up and met my eyes with something that might have been sympathy or might have been something else entirely. 'Mrs. Harper, I appreciate you bringing this to my attention,' she said. 'These electronic systems can be incredibly complex, and errors do happen. We take patient safety very seriously here.' I waited for more, but she just kept looking at me with that calm, measured expression. Then she leaned forward slightly. 'These are serious allegations—do you have any proof of intentional wrongdoing?'
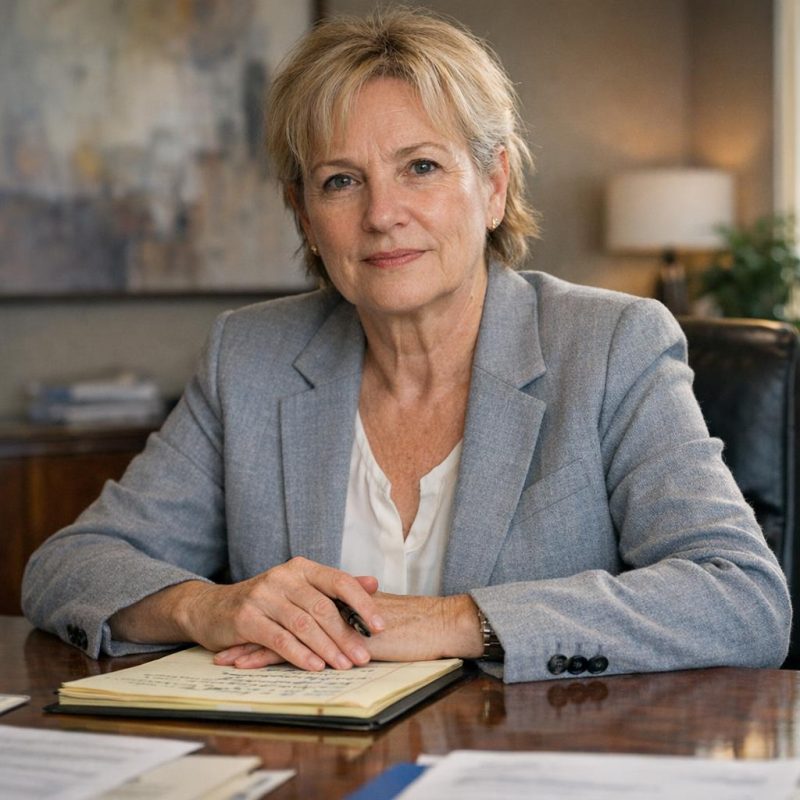 Image by RM AI
Image by RM AI
The Legal Threat
I opened my mouth to respond, but Sandra continued before I could speak. 'You see, Mrs. Harper, there's a significant difference between system errors and fraud. System errors are unfortunate but correctable. Fraud allegations, on the other hand, can be very damaging—not just to the institution, but to the person making them.' Her tone never changed, still perfectly professional, still wearing that concerned administrator expression. 'I'm sure you understand that making unsubstantiated accusations could constitute defamation. Especially if those accusations were to become public. We would be forced to protect the hospital's reputation, and that can get very complicated legally.' She smiled then, a small, tight smile that didn't reach her eyes. 'I'd hate to see someone acting out of genuine concern for their sister end up facing a lawsuit. These things can drag on for years, cost tens of thousands in legal fees.' She stood up, signaling the meeting was over. 'I'll have our IT department review the cases you've mentioned. We'll be in touch.' As I left her office, walking past the expensive art and the gleaming floors, I realized she'd just threatened me—politely, professionally, but unmistakably.
 Image by RM AI
Image by RM AI
Carla's Resistance
I drove straight to Carla's house. She was in the kitchen when I arrived, making tea with hands that still shook slightly from the medication adjustments. I told her about the meeting with Sandra, about the veiled threats, about how they were trying to intimidate me into silence. She set down her teacup with a clatter. 'Evelyn, please. Just stop.' Her voice was barely above a whisper. 'I know you're trying to help, but this is getting dangerous. These people have lawyers, they have money, they have power.' She wrapped her arms around herself like she was cold, even though the kitchen was warm. 'What if they come after us? What if they make our lives hell?' I started to say something about standing up to bullies, about doing what's right, but she cut me off. 'You have grandkids, Evelyn. I have a daughter. We're not investigative journalists, we're just regular people.' Tears were running down her face now. 'I'm scared. I'm really scared of what they might do.' And the worst part was, I couldn't promise her they wouldn't retaliate. I couldn't promise her we'd be safe. I couldn't even promise myself.
 Image by RM AI
Image by RM AI
The Insurance Company
But I couldn't just do nothing. The next day, I called Carla's insurance company and asked to speak with their fraud investigation department. I spent an hour on hold before reaching a tired-sounding woman named Patricia who listened to my explanation with what seemed like practiced patience. I described the merged records, the unnecessary procedures, the billing for conditions Carla didn't have. There was a long pause after I finished. 'Ma'am, can you tell me which hospital this occurred at?' Patricia asked. I told her. Another pause, the sound of typing. 'I see,' she said, and something in her tone made my stomach drop. 'We've actually received several similar reports from that facility over the past eighteen months. We've flagged it for review with our compliance team.' I felt a surge of hope—they already knew about it. But then she continued. 'These investigations can take quite a while to complete. Insurance fraud cases are complex, especially when they involve healthcare providers. We're looking at years, potentially, before any action could be taken.' Years. I thanked her and hung up, staring at the phone in my hand. She said, 'We've flagged this facility for review, but these investigations can take years.'
 Image by RM AI
Image by RM AI
The Medical Board
If the insurance company wouldn't act quickly, maybe the medical board would. I spent the entire next day preparing my complaint to the state medical board, organizing all of Jamie's documentation into a clear timeline, writing detailed descriptions of each case. I included copies of the merged records, the billing statements, the patterns I'd identified. I submitted it online and followed up with a phone call to their investigation department. The woman who answered sounded overwhelmed before I even started talking. She took down my information and gave me a case number. 'What happens next?' I asked. 'Someone will be assigned to review your complaint,' she said. 'They'll contact the facility for their response, review any documentation, possibly conduct interviews.' I asked how long that would take. Another pause. 'Our current backlog is significant. Most cases take between six and twelve months for initial review, depending on complexity.' My hand tightened on the phone. 'Six to twelve months?' 'At minimum,' she confirmed. I thanked her mechanically and ended the call. Six to twelve months—during which how many more patients would be harmed?
 Image by RM AI
Image by RM AI
The Online Campaign
That night, I sat down at my computer and started typing. I wrote about what happened to Carla—the routine admission that turned into a nightmare of wrong medications and false diagnoses. I described the merged medical records, the billing errors, the patterns I'd discovered. I was careful, very careful, to stick to facts I could prove. I didn't use the words 'fraud' or 'intentional.' I didn't accuse anyone by name. I just told the story and asked a question: 'Has this happened to you at Regional Medical Center?' I posted it to Facebook, tagged every local community group I could find, shared it to Twitter and a couple of healthcare forums I'd discovered. Then I closed my laptop and tried to sleep, though my mind kept spinning. The next morning, I woke up to seventy-three notifications. People had shared my post. They were commenting, tagging friends, telling me to check my messages. I opened my inbox—there were dozens of private messages from strangers, all starting the same way: 'This happened to me too.' Within hours, the post had been shared two hundred times—and I started getting messages from other victims.
 Image by RM AI
Image by RM AI
The Victims' Stories
I spent the next three days doing nothing but reading messages and conducting phone interviews. Every story followed a similar pattern, but each had its own nightmare details. A woman named Janet had been treated for kidney disease she didn't have, put on medications that made her actually sick. A man named Robert described being billed for surgical consultations he'd never attended, for conditions that appeared in his records after a simple check-up. A couple in their seventies told me about overlapping diagnoses, conflicting medications, nobody able to explain why their records showed medical history that wasn't theirs. I documented everything in a spreadsheet—names, dates, procedures, charges. The pattern was unmistakable now. These weren't isolated glitches. This was happening over and over, to dozens of people, maybe more. Some had complained and been told it was a computer error, quickly corrected. Others had just paid their bills and moved on, trusting that hospitals don't make those kinds of mistakes. Then I got a message from a man named David Torres. He wrote three sentences that made my blood run cold. One man told me he'd nearly died from a medication prescribed for a condition he didn't have—a condition that appeared in his merged records.
 Image by RM AI
Image by RM AI
The Common Thread
I printed out all the stories and spread them across my dining room table, looking for patterns beyond the obvious. There had to be something I was missing, some detail that would make this make sense. I started sorting them by demographics—age, gender, location. Nothing significant. Then I sorted them by the type of procedures: cardiology, oncology, endocrinology, orthopedics. Still nothing clear. Finally, I sorted them by payment method, and that's when I saw it. Out of forty-three detailed cases, forty-one had insurance coverage—and good insurance, the kind that covers expensive procedures with minimal pushback. The two exceptions were patients who'd later updated their records to include insurance information. I went back through each case, checking the billing amounts. The patients with comprehensive insurance were the ones getting the expensive tests, the specialist consultations, the high-cost interventions. I searched through my notes for any cases involving self-pay patients or people with Medicaid, the kind of coverage that questions every charge. There were none. Not one. Not in all the messages I'd received, all the stories I'd collected. That couldn't be a coincidence.
 Image by RM AI
Image by RM AI
The Pattern Recognition
I couldn't keep looking at paper anymore. I needed to see everything at once, in a way that made sense. So I opened a new spreadsheet and started entering every single case I'd collected—forty-three rows, each one representing someone who'd been through what Margaret experienced. I created columns for everything: age, procedure type, insurance provider, diagnostic category, total billing amount. It took me three hours to input all the data, triple-checking every entry. When I finished, I started filtering and sorting, looking for any pattern that might explain why these particular patients had been affected. The age distribution was random. The geographic spread across the hospital's service area was normal. But when I sorted by diagnostic category, something jumped out at me. Cardiology, oncology, neurology—the three most expensive specialties—accounted for thirty-seven of the forty-three cases. The high-value diagnostic categories. The ones where a single test could cost thousands, where specialist consultations ran into hundreds per visit, where insurance companies paid out substantial sums with relatively few questions. I added another column: average billing per case. The numbers were staggering. Each 'error' had generated between $8,000 and $47,000 in medical charges. I sat back and stared at the screen, my coffee going cold beside me. I stared at the data and felt something shift inside me—this wasn't incompetence, this was something else entirely.
 Image by RM AI
Image by RM AI
The Journalist
The message came through LinkedIn two days later. 'Ms. Chen, my name is David Rosenberg. I'm an investigative journalist with the County Register. I've been following your posts about your sister's medical records issue and the community response you've generated. I'd like to discuss this with you. Would you be available for a call?' I looked him up immediately. Twenty years of healthcare reporting, two state journalism awards, a track record of holding institutions accountable. I called him that afternoon. He was direct but careful. 'I want to be clear,' he said. 'I'm not looking to sensationalize anything. But the pattern you've documented—if it's what it appears to be—that's a story that needs to be told.' We talked for over an hour. I shared everything: the original error, Margaret's experience, the forty-three cases I'd collected, the insurance pattern I'd just identified. He asked detailed questions, taking notes, occasionally going quiet in a way that made me think he was seeing the same thing I was seeing. At the end of the call, his voice changed slightly. More serious. More focused. He said, 'If what you're suggesting is true, this could be one of the biggest healthcare fraud cases in state history.'
 Image by RM AI
Image by RM AI
The Investigation Begins
David moved fast. Within a week, he'd filed public records requests with the state health department and the hospital's corporate parent company. He started making calls—former employees, current staff who'd speak off the record, medical billing experts, healthcare policy analysts. He'd update me every few days, sharing what he could without compromising his sources. The picture that emerged was disturbing. Three former employees corroborated that 'system errors' had been an ongoing problem for at least two years, maybe longer. A medical coder who'd left six months ago told him she'd raised concerns about the unusual number of record mergers in high-value diagnostic categories and was told it was 'just a software glitch they were working on.' A nurse who'd transferred to another hospital said she'd questioned why so many patients were being scheduled for unnecessary follow-ups based on diagnoses that didn't match their symptoms. She was written up for 'undermining physician authority' and advised to 'focus on her own responsibilities.' David's voice was grim when he shared that particular interview. One former nurse told him, 'We all knew something was wrong, but anyone who spoke up got fired or transferred.'
 Image by RM AI
Image by RM AI
The Attorney
David called me on a Friday afternoon. 'I want you to meet someone,' he said. 'Her name's Lisa Chen—no relation, I checked—and she's a healthcare fraud attorney. She's handled cases against hospitals, pharmaceutical companies, medical device manufacturers. I showed her what we've collected so far. She wants to talk.' We met at a coffee shop downtown the next morning. Lisa was younger than I expected, maybe late thirties, with the kind of focused intensity that made me think she didn't miss much. She'd brought her laptop and pulled up a document as soon as we sat down. 'I've reviewed everything David shared with me,' she said. 'The pattern is clear. The financial motive is obvious. What you've documented could absolutely support a fraud case.' My heart started pounding. 'But?' I asked, because there's always a but. She nodded. 'Healthcare fraud requires proof of intent. We'd need to show the hospital knew about the problem and deliberately allowed it to continue—or worse, engineered it—for financial gain. Right now, what we have could be argued as negligence, incompetence, or just bad software implementation. Those are civil matters with much smaller penalties.' She closed her laptop and looked directly at me. Lisa said, 'But we need a smoking gun—something that proves intent, not just negligence.'
 Image by RM AI
Image by RM AI
The Informant
Jamie's text came at 11:47 PM on a Tuesday. 'Can we meet? Found something important. Not safe to discuss digitally.' We met in the parking lot of a 24-hour diner on the edge of town, away from the hospital, away from anywhere we might be recognized. He looked like he hadn't slept in days. Dark circles under his eyes, his usually neat appearance rumpled and stressed. 'I shouldn't be doing this,' he said as soon as he got in my car. 'I could lose my job. Worse, probably.' I waited. He pulled a manila envelope from his jacket and held it for a moment before handing it over. 'I was doing routine maintenance on archived emails last week. Part of my job is making sure the system's running efficiently, clearing out old data according to retention policies. I found these in a folder that should have been deleted months ago. Someone marked them for preservation—probably by accident.' Inside were printouts of internal emails. I started reading the first one and felt my hands go cold. Subject line: 'Q3 Performance Enhancement.' Body text discussing the patient matching algorithm's 'revenue optimization features' and the need to 'maximize diagnostic yield while maintaining plausible deniability.' He was shaking when he handed me the printouts and said, 'This could cost me everything.'
 Image by RM AI
Image by RM AI
Revenue Optimization
I stayed up all night reading through the emails Jamie had given me. There were seventeen in total, spanning about eight months. Most were between Sandra Morrison and the IT director, with occasional input from someone in finance. The language was careful—corporate and vague in places—but the meaning became clearer with each message. They discussed 'adjusting matching parameters to optimize patient flow through diagnostic services.' They talked about 'threshold sensitivity' and 'false positive tolerance levels.' In one email, the IT director explained how lowering the matching threshold would 'increase merge events' which would 'naturally drive additional diagnostic testing to resolve ambiguities.' Another email referenced a consultant's report about 'revenue capture opportunities in high-value service lines.' The most damning exchange happened in September. Sandra had written: 'Our cardiology and oncology numbers are down for Q3. The board is asking questions. What can we do on the systems side to improve capture rates?' The IT director's response came three hours later: 'We can adjust the algorithm's sensitivity in those diagnostic categories. Estimated increase in diagnostic testing: 15-20%. Implementation timeline: 2 weeks.' One email from Sandra to the IT director said: 'We need to improve our Q3 numbers—can we adjust the sensitivity?'
 Image by RM AI
Image by RM AI
The Second Set of Files
Jamie contacted me again four days later. This time he didn't ask to meet in person—he just showed up at my front door at seven in the morning with another envelope, thicker than the first. 'I'm done,' he said. 'I already gave my two weeks' notice. After you see what's in here, you'll understand why.' These documents were different. Internal audit reports from the hospital's compliance department, dated six and nine months ago. Both audits had identified the same problem: an unusually high rate of patient record mergers in specific diagnostic categories, resulting in documented cases of incorrect diagnoses and inappropriate testing. The recommendations were clear: suspend the algorithm, conduct a thorough review, implement stricter matching criteria, notify affected patients. But attached to each audit report was a response memo from administration. The first memo acknowledged the findings but stated that 'the cost and operational disruption of suspending the system outweighs the relatively small number of affected patients.' The second memo was more explicit. It included a financial analysis prepared by an outside consulting firm. The last document was a cost-benefit analysis that calculated potential legal settlements against increased revenue—and recommended staying the course.
 Image by RM AI
Image by RM AI
The Truth Revealed
We met in Lisa's office—me, David, and Lisa herself, with all the evidence spread across her conference table. Lisa had spent three days reviewing every document, every email, every piece of data we'd collected. Now she stood at the head of the table with a timeline she'd created, walking us through what the evidence proved. 'Here's what happened,' she said. 'The hospital implemented a new records system with a patient-matching algorithm. They quickly realized the algorithm generated false matches—merging records of different patients with similar names or demographics. Instead of fixing it, they saw an opportunity.' She pointed to the emails. 'They deliberately adjusted the algorithm's matching parameters to increase false positives in high-value diagnostic categories—cardiology, oncology, neurology. Each false match created diagnostic ambiguity: suddenly a patient had a history they'd never actually had. Doctors, acting in good faith on incorrect records, would order tests to investigate these phantom conditions. The hospital billed insurance for thousands of dollars in unnecessary procedures. When patients questioned it, staff had rehearsed responses: software glitch, unfortunate error, happens sometimes. Meanwhile, internal audits identified the problem twice, and both times administration chose to continue because the revenue exceeded their projected legal liability.' Lisa looked at both of us. This wasn't a series of unfortunate errors—it was systematic fraud built into the system from the beginning.
 Image by RM AI
Image by RM AI
The Realization
Sitting alone in my living room that night after Lisa's presentation, I kept replaying every moment from Carla's hospital stay, and suddenly everything made sense. The lab tech who'd been so nervous when I asked about the blood work—she knew the records were wrong, must have seen it in the system and been told to keep quiet. Those rehearsed answers Sandra and her staff gave when I questioned inconsistencies—they weren't scrambling to cover individual mistakes, they were following a script they'd developed specifically for situations like mine. The way Jamie had looked physically ill when showing me the merged records—he'd known exactly what he was seeing, had probably seen it dozens of times before. Even Nurse Bailey's careful warnings about 'being my own advocate'—she'd been trying to tell me the system itself couldn't be trusted. Every defensive response, every deflection, every 'this sometimes happens' had been deliberate. They weren't trying to fix a problem or prevent future errors. They were protecting a revenue stream. The hospital had weaponized the confusion itself, knowing that most patients would eventually give up, pay the bills, and move on with their lives. Most people don't have the time, energy, or resources to fight a hospital's billing department for months. And here's what made my stomach turn: they'd done this to hundreds, maybe thousands of patients, and gotten away with it because no one thought to question the system itself.
 Image by RM AI
Image by RM AI
Building the Case
The next two weeks were a blur of coordination and preparation. Lisa rented a larger office space to handle the case, with whiteboards covering every wall showing timelines, victim names, and evidence connections. David set up camp in one corner, interviewing victims for his article and cross-referencing their stories with the internal documents we'd obtained. I became the unofficial coordinator, spending hours on the phone with people who'd experienced the same nightmare Carla had—unnecessary cardiac workups, oncology referrals for cancers they'd never had, neurological tests based on phantom symptoms in falsified records. Each person I spoke with had the same story: confusion, ruinous bills, and staff responses that now sounded chillingly familiar. Lisa worked eighteen-hour days, building the legal framework for a class-action suit while documenting every piece of evidence with meticulous precision. 'We need this airtight,' she'd say, reviewing documents at midnight with her reading glasses sliding down her nose. Then the hospital struck back—a legal messenger delivered a thick envelope to Lisa's office one Tuesday morning. Inside was a cease-and-desist letter threatening legal action if we continued 'making defamatory statements' about the hospital's operations. I watched Lisa read it, expecting concern, maybe even hesitation. Instead, she smiled—actually smiled—looked up at David and me, and said, 'Let them try to stop us.'
 Image by RM AI
Image by RM AI
The Article Drops
David's article hit the paper's website at 6 AM on a Thursday, and by the time I woke up at seven, my phone was already exploding with notifications. The headline read: 'Local Hospital Systematically Defrauded Patients Through Falsified Medical Records, Internal Documents Reveal.' He'd laid it all out—the algorithm manipulation, the internal audits that were ignored, the rehearsed responses staff gave to victims. He quoted from Sandra's emails, included testimony from a dozen victims, and reproduced some of Jamie's documentation showing the scope of false matches. The comments section filled within minutes, hundreds of people sharing their own experiences or tagging friends who'd had similar issues at the same hospital. David had also secured statements from two healthcare billing experts who called it 'one of the most calculated fraud schemes they'd encountered in modern hospital administration.' Local TV stations started calling me for interviews before 8 AM. The paper's website crashed twice from traffic volume. By noon, the story had been picked up by the Associated Press and was running on news sites across the country. My sister called, crying, saying she'd finally been believed. And then, at 3 PM, David called me with news that made everything real in a way it hadn't been before: 'Evelyn, turn on the news. The state attorney general's office just announced they're opening a criminal investigation.'
 Image by RM AI
Image by RM AI
The Media Storm
The story went absolutely viral. Within forty-eight hours, I'd been interviewed by three local news stations, two national cable networks, and a healthcare podcast with over a million listeners. CNN ran a segment calling it 'a cautionary tale about the digitization of medical records without proper oversight.' Social media exploded with people sharing their own hospital billing nightmares, many specifically mentioning the same facility or its parent corporation. The hospital tried to respond with carefully crafted statements about 'taking these allegations seriously' and 'conducting our own internal review,' but you could see the panic in their PR strategy—they were deleting social media posts, restricting comments, and their carefully curated Facebook page became a disaster zone of angry former patients. I watched it unfold with this strange mixture of vindication and exhaustion. Then on Saturday evening, Sandra herself appeared on the local news for a live interview. She wore a navy blazer and pearl necklace, her makeup professionally done, sitting in what looked like her home office with medical textbooks visible behind her. The interviewer asked direct questions about the fraud allegations, the internal emails, the victims' testimony. Sandra denied everything with practiced responses: 'These allegations are grossly exaggerated,' she said, her voice steady and calm. But I noticed something the cameras caught, too—her hands were shaking the entire interview.
 Image by RM AI
Image by RM AI
The Walkout
The hospital's facade started crumbling from the inside. On Monday morning, Nurse Bailey held a press conference outside the hospital's main entrance, flanked by six other nurses and medical staff. She read from a prepared statement, her voice clear and unwavering: 'I'm resigning my position effective immediately. For too long, I've watched patients suffer because of record-keeping practices I knew were wrong. I can no longer be complicit in a system that prioritizes billing revenue over patient safety.' The other nurses nodded in agreement, several visibly emotional. Then Jamie stepped forward—I'd been in touch with him throughout the legal preparation, but seeing him go public took real courage. He'd brought copies of internal communications, evidence he'd quietly preserved knowing this day might come. 'I was told repeatedly to ignore record discrepancies,' he told the assembled reporters, his voice shaking slightly but determined. 'Administration knew the system was generating false matches and chose to let it continue because it was profitable. I couldn't be part of it anymore—not after seeing what they did to people.' By that evening, twelve more staff members had submitted resignations, and three doctors had requested transfers to other facilities. The hospital released a statement calling the walkout 'unfortunate' and 'based on misunderstandings,' but nobody was buying it anymore. Jamie told reporters afterward, his words broadcast on the evening news: 'I couldn't be part of it anymore—not after seeing what they did to people.'
 Image by RM AI
Image by RM AI
The Investigation Expands
The state investigation had barely begun when federal authorities showed up. Lisa called me on a Wednesday afternoon, her voice carrying an edge I'd never heard before—not quite excitement, but something close. 'The FBI just contacted me,' she said. 'They want to see all our evidence. The Department of Justice is getting involved.' Apparently, once federal investigators started looking at the hospital's parent corporation, they found something that made our local case look like just the beginning. The corporation, MedStar Health Systems, owned seventeen hospitals across Pennsylvania, Ohio, and West Virginia. Investigators found identical algorithm manipulation at facilities in all three states—the same deliberately adjusted matching parameters, the same rehearsed staff responses, the same pattern of ignored internal audits. It wasn't a rogue hospital administrator making bad decisions. It was corporate policy, implemented systematically across multiple states, generating an estimated forty-seven million dollars in fraudulent billing over three years. Lisa showed me the federal filing—pages and pages of evidence showing coordinated fraud at the corporate level, with emails between executives discussing 'diagnostic ambiguity revenue streams' and 'acceptable risk thresholds for patient complaints.' I sat in her office, staring at those documents, feeling sick. All those months I'd been fighting for Carla, thinking we were dealing with one hospital's incompetence, one administrator's greed. This wasn't just one hospital—it was a nationwide operation.
 Image by RM AI
Image by RM AI
The Class Action Filed
Lisa filed the class-action lawsuit on a Monday morning at the federal courthouse, and she'd invited me to be there when she did it. The filing was over two hundred pages long, representing three hundred and seventeen victims across four states, with documented damages totaling over six million dollars in fraudulent charges alone—not counting the emotional distress, the medical complications from unnecessary procedures, or the financial devastation many families had experienced. The lawsuit named MedStar Health Systems, the local hospital, Sandra, and four corporate executives as defendants. It demanded full restitution for all victims, punitive damages to discourage future fraud, and criminal prosecution of everyone involved in implementing and maintaining the scheme. But the part that made me actually hopeful was the request for immediate relief: Lisa had included a motion for a temporary restraining order requiring the hospital to shut down its current records system immediately and implement independent oversight of all patient records pending trial. 'We're not just asking for compensation,' Lisa explained to the reporters gathered on the courthouse steps. 'We're asking the court to stop this from happening to anyone else, right now, today.' She handed me a copy of the filing, and I held that thick document in my hands, thinking about all the victims whose stories were documented inside it, all the people who'd thought they were alone until David's article gave them permission to come forward. The filing included a request for a temporary restraining order to shut down the hospital's records system immediately.
 Image by RM AI
Image by RM AI
The Arrests
The arrests happened on a Thursday morning, coordinated across three states simultaneously. I was at home when Lisa called: 'Turn on the news. It's happening.' I switched on the television just in time to see Sandra being led out of the hospital's administrative building in handcuffs, two FBI agents flanking her while cameras caught every moment. She wasn't wearing her usual polished administrator outfit—they'd arrested her at home early that morning, and she was still in casual clothes, her hair unstyled, her face pale and shocked. The news anchor explained that she and seven other executives had been arrested on charges of healthcare fraud, conspiracy to commit fraud, and racketeering. Federal prosecutors were seeking significant prison time, asset forfeiture, and permanent bans from healthcare administration. I watched Sandra being guided into a federal vehicle, her hands cuffed behind her back, and waited for the rush of triumph I'd imagined feeling at this moment. It didn't come. Instead, I just felt profoundly tired—tired from months of fighting, tired from reliving Carla's trauma over and over while helping other victims document theirs, tired from carrying the weight of knowing how many people had been hurt by a system that was supposed to heal them. Justice was happening, yes, but it couldn't undo what had been done. Watching Sandra being led away in handcuffs, I felt something I hadn't expected—not triumph, but exhaustion.
 Image by RM AI
Image by RM AI
The System Shutdown
The federal judge granted the restraining order on a Friday afternoon, and by Monday morning, the hospital's entire automated records system had been shut down. I was there when it happened—Lisa had invited me to witness it, said I'd earned the right to see this moment. Kumar, the IT director who'd testified about the system's flaws, stood in the server room with two federal monitors, methodically disabling the algorithms that had merged and corrupted so many patient files. He looked exhausted, like he'd aged ten years in the months since the investigation began. 'We're essentially going back to paper until we can verify every single record,' he explained to the monitors. 'Every patient file that was touched by the automated system needs manual review.' I asked how long that would take. He rubbed his eyes, then pulled up a spreadsheet showing the scope: forty-seven thousand patient records potentially affected, each requiring individual audit. 'Months,' he said. 'Maybe a year. And even then...' He trailed off, but I understood what he wasn't saying. Some of the damage was permanent—treatment decisions made based on wrong information, medications given or withheld because files were merged, diagnoses missed because symptoms were attributed to the wrong patient. You can't un-ring that bell, can't undo treatments that happened months ago. Kumar testified that it would take months to untangle all the merged records—and even then, some damage might be irreversible.
 Image by RM AI
Image by RM AI
The Aftermath
Six months later, I sat with Carla at her kitchen table, both of us reviewing settlement offers from the hospital's insurance company. The envelope had arrived that morning, official and thick with legal documents. Carla's hands were steadier now than they'd been in the hospital—physical therapy had helped, and her actual medical conditions were finally being properly treated. She'd gained back some of the weight she'd lost, and there was color in her face again. But I could still see the toll everything had taken, the way she flinched slightly when medical bills arrived in the mail, how she triple-checked every piece of correspondence from her doctors. The settlement amount was substantial—six figures, more money than either of us had seen in one place before. It covered her medical expenses, the treatments she'd been denied, compensation for pain and suffering. The lawyers said it was a good offer, that the class action would likely yield similar amounts for other victims. I watched Carla read through the terms, her finger tracing each line carefully. She'd learned to read everything thoroughly now, to trust nothing at face value. When she reached the final page, she set the papers down and looked at me with those same eyes I'd seen in the hospital room all those months ago, eyes that had learned too much about how systems can fail the people they're supposed to protect. Carla looked at the settlement amount and said quietly, 'Is this enough for what they put people through?'
 Image by RM AI
Image by RM AI
The New Normal
I've become someone I never expected to be—an advocate for healthcare transparency, speaking at medical conferences and working with state legislators to strengthen patient protections. Last month, I testified before a congressional committee about the need for federal oversight of hospital AI systems. It's meaningful work, important work. I've helped draft legislation that would require independent audits of automated medical records systems, mandate patient notification when AI is used in treatment decisions, establish penalties for hospitals that suppress safety concerns. Three states have already passed versions of the bill. I get emails now from people across the country who've noticed inconsistencies in their medical records, who've felt dismissed by doctors, who've had that same nagging sense that something wasn't right. I try to help each one, connecting them with patient advocates, explaining how to request full records, teaching them the questions I learned to ask. Some of them uncover problems. Most don't—most of the time, it really is just a routine issue, a clerical error, nothing sinister. But the act of asking, of paying attention, of refusing to accept 'don't worry about it' as an answer—that matters. Carla's doing better, and the hospital has implemented new safeguards, and Sandra's awaiting trial on multiple federal charges. Justice happened, or as close to it as we're likely to get. But late at night, I still think about all the people who weren't lucky enough to have someone ask questions on their behalf.
 Image by RM AI
Image by RM AI
The Question That Started Everything
Looking back now, I realize that everything changed because of one decision: I stayed. I didn't go home when the doctors said Carla was fine. I didn't accept the polite explanations that didn't quite add up. I paid attention to details that seemed small—a nurse's hesitation, an inconsistent timeline, medications that didn't match the diagnosis. I asked questions even when the asking felt uncomfortable, even when people made it clear I was being inconvenient. That's what I've learned from all of this: systems count on our politeness, our deference to authority, our willingness to believe that surely someone else is paying attention. They count on us accepting 'routine' and 'standard procedure' and 'nothing to worry about' without pushing back. Most of the time, those reassurances are true. But sometimes they're not, and the only way to know the difference is to ask. Carla and I talk about it now, sitting at her kitchen table with tea, processing everything that happened. She's forgiven me for the times I pushed too hard, and I've forgiven myself for the moments I almost gave up. We're both different people than we were that Tuesday morning when she went in for what was supposed to be a routine issue. Stronger, maybe. Definitely more skeptical. Permanently changed. I tell Carla now: never stop asking questions, especially when someone makes it seem like you shouldn't—because sometimes one small question can uncover something much bigger than either of us ever expected.
 Image by RM AI
Image by RM AI
KEEP ON READING

The Love Story Behind the Taj Mahal Was Also a…
Koushik Chowdavarapu on UnsplashThe Taj Mahal is often introduced as…
By Emilie Richardson-Dupuis Apr 2, 2026
JFK's Last Meal Is A Testament To His Character
Walt Cisco, Dallas Morning News on WikimediaHistory often focuses on…
By Sara Springsteen Apr 2, 2026
Public Executions Were Once the Most Attended Events in Town…
Georg Heinrich Sieveking on WikimediaFor centuries, a public execution could…
By Breanna Schnurr Apr 2, 2026
20 Old Hollywood Feuds That Went Beyond The Studio Lot
When The Smiles Stopped. Old Hollywood sold a polished fantasy,…
By Breanna Schnurr Apr 2, 2026
The Coup Triggered by a Pop Song
Matheus Ferrero on UnsplashMost political upheavals have a trigger that…
By Cameron Dick Apr 2, 2026
How The Black Death Spurred the Renaissance
Art Institute of Chicago on UnsplashThe Black Death, which swept…
By Rob Shapiro Apr 2, 2026